 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
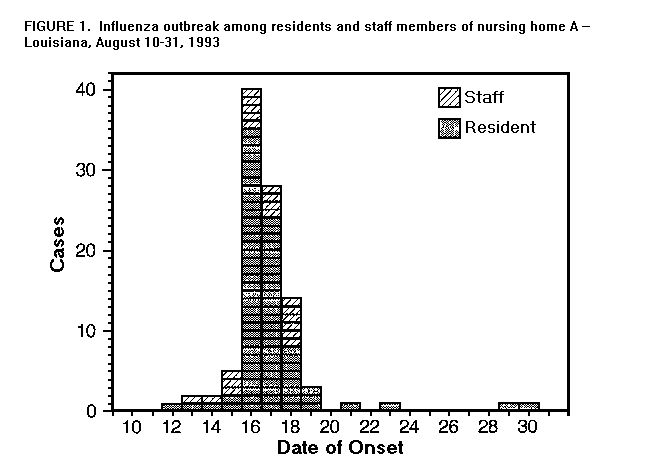
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influenza A Outbreaks -- Louisiana, August 1993In August 1993, the Louisiana Department of Health and Hospitals (LDHH) investigated reports of acute respiratory illness among residents of two nursing homes and workers on a dredging barge in southern Louisiana; influenza type A has been confirmed as the cause of these outbreaks. This report summarizes the investigations of the outbreaks. Outbreak 1 On August 18, 1993, LDHH initiated an investigation of an outbreak of acute respiratory illness in nursing home A in southeastern Louisiana. During August 12-August 30, 79 (64%) of 124 residents of this nursing home had acute respiratory illness (Figure_1), of whom 40 had a documented temperature greater than or equal to 100 F {37.8 C} and cough. The 79 ill residents ranged in age from 34 to 99 years (median: 81 years). Onset of similar symptoms was reported by 20 of 100 staff members during the same period; the ages of ill staff members ranged from 22 to 55 years (median: 36 years). Twenty-five ill residents were hospitalized; two had radiographic signs of pneumonia. Nasopharyngeal swabs obtained from nine residents and staff were cultured. Influenza type A was isolated from four of these cultures. Antigenic characterization of two of these indicated that the hemagglutinin was most closely related to the A/Beijing/ 32/92(H3N2) strain circulating at the end of the 1992-93 influenza season and included in the 1993-94 influenza vaccine. LDHH advised nursing home A to minimize contacts between residents. Amantadine was not used because influenza type A was not considered a likely etiologic agent at the time of the outbreak. Outbreak 2 On August 20, LDHH initiated an investigation of an outbreak of acute respiratory illness at nursing home B in southwestern Louisiana affecting 26 (46%) of 57 residents; 10 of 40 employees also reported illness. Ill residents ranged in age from 34 to 92 years (median: 84 years); ill employees ranged in age from 22 to 62 years (median: 37.5 years). Of the 26 ill residents, 25 (96%) had cough, 24 (92%) had fever, and 19 (73%) had headache. Two employees were hospitalized. Five of five paired acute- and convalescent-phase serum specimens showed a fourfold or greater rise in antibody titer to influenza type A by complement fixation. LDHH advised restricting contact between residents. Outbreak 3 On September 2, LDHH received a report of acute respiratory illness among persons living and working on a dredging barge anchored in a southeastern Louisiana river. Of 51 persons who had worked on the barge for some period during August 25-September 3, 28 (55%) had onset of illness consisting of cough (89%), fever (82%), headache (82%), myalgias (82%), or sore throat (79%). Ill persons ranged in age from 19 to 63 years (median: 36 years). Four were hospitalized. Influenza type A was isolated from cultures obtained from five ill persons. Subtyping of this isolate and further investigation of this outbreak are under way. LDHH recommended that ill persons continuing to stay on the barge be housed separately from well persons. Amantadine was administered for treatment to all ill persons and for prophylaxis to well persons remaining on the barge. Since the start of amantadine, only one additional person has become ill on the barge. Surveillance for Influenza-Like Illness in Other Sites On September 1, active surveillance for influenza-like illness (ILI) was initiated throughout Louisiana. LDHH contacted 116 (34%) of the 343 nursing homes in the state; all 59 nursing homes in the regions where outbreaks 1-3 occurred and 57 of the remaining nursing homes in the state; a total of 12,026 persons reside in these facilities. Twelve nursing homes reported cases of acute respiratory illness with cough, fever, or myalgias among residents during the preceding month. These reports included cases in 56 residents. The highest attack rate in any of these facilities was 7.5%; three residents required hospitalization. As part of the active surveillance, LDHH also contacted nine hospital emergency departments and nine sentinel physicians around the state. Three hospital emergency departments reported a total of 23 patients with ILI during the month of August, one of whom was hospitalized. One physician located in the southeastern region of the state, but distant from these three outbreaks, reported five patients with ILI. Reported by: C Bolotte, MD, H Louviere, T Foret, K Butler, Napoleonville; B Holden, MD, K Fruge, J Stewart, Crowley; W Johnson, MD, A Wiltz, C Granger, Morgan City; D Sundin, PhD, AP Causey, Charity Hospital, New Orleans; S Wilson, K Kelso, MS, R Tapia, MPH, Epidemiology Section, L McFarland, DrPh, State Epidemiologist, H Bradford, Jr, PhD, Bur of Laboratory Svcs, Office of Public Health, Louisiana Dept of Health and Hospitals. Influenza Br and Epidemiology Activity, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Div of Field Epidemiology, Epidemiology Program Office, CDC. Editorial NoteEditorial Note: Although sporadic cases of influenza may occur in the United States throughout the year, outbreaks of influenza during the summer are rare. This report describes three laboratory-confirmed influenza type A outbreaks that occurred in southern Louisiana during August and early September. Antigenic characterization of the hemagglutinin of two of the viruses isolated in these outbreaks indicates they are similar to the influenza A/Beijing/32/92(H3N2) strain that circulated in the United States late last season. This strain has been included in the 1993-94 influenza vaccine. The unusual occurrence of outbreaks of confirmed and suspected influenza in August and early September has raised the question of whether influenza vaccine should be administered earlier this year than is usually recommended. To maximize opportunities for vaccinating high-risk patients, beginning in September such persons should be offered influenza vaccination during routine health care or when hospitalized. However, the recommendations of the Advisory Committee on Immunization Practices (ACIP) also state that the optimal time for organized vaccination programs for persons in high-risk groups is usually from mid-October through mid-November (1), so that the highest level of vaccine-induced antibody and protection are most likely to coincide with the highest levels of influenza activity in the United States -- which usually occurs from December through March. Because vaccine-induced antibody titers can begin to wane within several months of vaccination, if vaccine is administered too early, some persons who do not mount a high antibody response may have antibody titers that have declined below protective levels before influenza activity ends. The ACIP also recommends that vaccination programs can be initiated as soon as vaccine is available if regional influenza activity is expected to begin earlier than December (1). Because of the outbreaks described in this report, CDC has recommended that surveillance for influenza activity in other states begin as soon as possible to assist in determining whether vaccination should be encouraged earlier in other areas of the country. Early vaccination may be recommended nationally should laboratory-confirmed sporadic cases or outbreaks appear in several other areas of the country. In early September, CDC distributed influenza reagent kits to the 60 World Health Organization collaborating laboratories located throughout the United States to facilitate the identification of influenza viruses. Another measure for control of influenza type A is the use of an antiviral agent. Two antiviral agents with specific activity against influenza type A -- amantadine hydrochloride and rimantadine hydrochloride -- have been used for control of influenza type A. Only amantadine is licensed for use in the United States; however, rimantadine may be approved in time for use during the 1993-94 influenza season. Amantadine is recommended for prophylaxis and treatment of influenza type A infection under a variety of circumstances (2). These recommendations are available by facsimile through the CDC Voice Information System, telephone (404) 332-4555. Updated antiviral recommendations that may include rimantadine will be published separately later in the fall of 1993. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}