 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
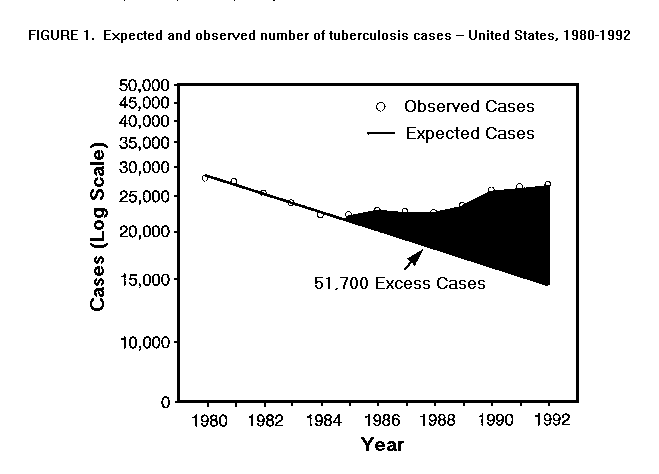
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Morbidity -- United States, 1992In 1992, 26,673 cases of tuberculosis (TB) (10.5 cases per 100,000 population) were reported to CDC from the 50 states, the District of Columbia, and New York City *, a 1.5% increase over the number reported in 1991 (26,283 {10.4 cases per 100,000}). In addition, 370 cases were reported from Puerto Rico (312) and the U.S. territories (58). This report summarizes final TB surveillance data for 1992 and compares findings with previous years. During 1992, 22 states reported increases over 1991 in the number of TB cases. The largest increases occurred in Virginia (20.6%), Illinois (6.5%), New York (including New York City) (3.3%), and California (2.1%). The largest increases reported in cities with populations of 250,000 or more were in Houston (25.7%), San Diego (19.3%), Chicago (5.9%), and New York City (3.5%). From 1985 (the year with the lowest number of reported TB cases since reporting began) through 1992, reported TB cases increased 20.1%, from 22,201 to 26,673, respectively. During this period, the largest increases occurred in New York (84.4%), California (54.2%), and Texas (32.7%). If the trend of decline observed from 1980 through 1984 had continued through 1992, approximately 51,700 fewer cases would have been expected during 1985-1992 than were reported (Figure_1). From 1985 through 1992, reported TB cases increased in every racial/ethnic group except non-Hispanic whites and American Indians/Alaskan Natives (Table_1). Reported cases increased among Hispanics by 74.5%, among Asians/Pacific Islanders by 46.2%, and among non-Hispanic blacks by 26.8%. Cases decreased by 23.2% among American Indians/Alaskan Natives and by 9.9% among non-Hispanic whites. Compared with 1985, the number of reported TB cases increased for all age groups except for the greater than or equal to 65-year age group (Table_1). The largest increase occurred in the 25- 44-year age group (54.5%). A higher proportion of cases occurred among persons in younger age groups. From 1985 through 1992, the TB case rate in nonurban areas of the United States decreased from 6.7 cases per 100,000 to 6.5 (3.0%). In comparison, the rate in urban areas increased from 17.1 cases per 100,000 to 22.0 (28.6%). From 1986 (the first year in which all states reported the country of origin for persons with TB) through 1992, reported cases among foreign-born persons ** increased 47.6%. As a proportion of total reported cases, reported cases among foreign-born persons increased from 21.6% in 1986 to 27.3% in 1992. Of cases reported in 1992 among foreign-born persons whose year of arrival was known (83.6%), 58% had been in the United States for 5 years or less. Reported by: Div of Tuberculosis Elimination, National Center for Prevention Svcs, CDC. Editorial NoteEditorial Note: In 1992, TB cases increased among some racial/ethnic minorities, among foreign-born persons, and among persons aged 25-44 years and less than or equal to 15 years. The increases among Hispanics, non-Hispanic blacks, and Asians/Pacific Islanders primarily reflect the greater occurrence of TB among 1) persons infected with human immunodeficiency virus (HIV), 2) persons immigrating from countries with a high incidence of TB, and 3) primary transmission in these groups (1-8). Other contributing factors include socioeconomic factors such as substance abuse, limited access to health care, poverty, substandard housing, and homelessness (9). The increase in the 25-44-year age group and in urban areas is related, at least in part, to HIV infection. Results from CDC-funded unlinked surveys in TB clinics showed an HIV prevalence of 47% in 25-44-year-old U.S.-born patients (CDC, unpublished data, 1991). Increasing rates of TB among children aged less than or equal to 15 years may reflect increasing rates of transmission of Mycobacterium tuberculosis among adults. Among persons coinfected with M. tuberculosis and HIV, the risk for developing active TB is substantially increased because of HIV-related immunosuppression (4). Since 1989, the Advisory Committee for the Elimination of Tuberculosis has recommended that HIV-infected persons be screened for TB and latent TB infection and, if infected, be offered appropriate curative or preventive therapy (3). In addition, persons with TB and tuberculin skin test-positive persons should be evaluated for HIV infection to enable initiation of appropriate counseling and treatment (3). Since January 1993, results of HIV testing of TB patients have been collected on the confidential TB case-report form (Report of a Verified Case of Tuberculosis form). CDC also has been conducting HIV serosurveys in TB clinics since 1988 (5). These data will assist in more accurately determining the impact of HIV infection on TB morbidity trends in the United States. To determine factors responsible for the increasing trends, CDC, in collaboration with state and local health departments, has expanded TB surveillance to include additional information on risks for acquiring TB (including immunosuppression) and for nonadherence to therapy, drug-susceptibility results, and outcomes of therapy. In addition, state and local health departments have been encouraged to implement active surveillance for TB cases. In 1993, six state and local health departments have initiated programs to assess completeness of reporting of TB cases. Their findings can assist other health departments in developing strategies to improve the completeness of reporting, communicate with reporting sources, correct deficiencies in health-care provider knowledge about reporting TB, and improve diagnostic evaluation of suspect TB cases. References
* New York City is a separate reporting area.
** Persons born outside the United States and its territories.
TABLE 1. Reported cases and rates of tuberculosis, by sex, age group, race/ethnicity,
and country of origin -- United States, 1985 and 1992
=================================================================================================
No. cases Rate *
---------------- % ------------- %
Characteristic 1985 1992 Change 1985 1992 Change
-----------------------------------------------------------------------------------------------
Sex
Male 14,496 17,433 +20.3 12.5 14.0 +12.0
Female 7,704 9,236 +19.9 6.3 7.1 +12.7
Unknown 1 4 -- + NA & NA
Age group (yrs)
O- 4 789 1,074 +36.1 4.4 5.5 +25.0
5-14 472 633 +34.1 1.4 1.7 +21.4
15-24 1,672 1,974 +18.1 4.2 5.5 +31.0
25-44 6,758 10,444 +54.5 9.2 12.7 +38.0
45-64 6,138 6,487 + 5.7 13.7 13.4 - 2.1
>=65 6,356 6,025 - 5.2 22.3 18.7 -16.1
Unknown 16 36 -- NA NA
Race/Ethnicity
White, non-Hispanic 8,453 7,618 - 9.9 4.5 4.0 -11.1
Black, non-Hispanic 7,592 9,623 +26.8 23.0 31.7 +37.8
Hispanic @ 3,092 5,397 +74.5 21.4 22.4 + 4.7
Asian/Pacific Islander 2,530 3,698 +46.2 41.6 46.6 +12.0
American Indian/
Alaskan Native 397 305 -23.2 18.9 16.3 -13.8
Unknown/Other ** 137 32 -- NA NA
Country of origin ++
Foreign-born && 4,925 7,270 +47.6 NA NA
U.S.-born 17,712 19,225 + 8.5 NA NA
Unknown 131 178 -- NA NA
Total 22,201 26,673 +20.1 9.3 10.5 +12.9
-----------------------------------------------------------------------------------------------
* Per 100,000 population. Population by race/ethnicity are projections obtained from the
Bureau of Census (Source: Bureau of Census, Current population reports; series P-25, no.
1092, November 1992).
+ Not calculated.
& Denominator data not available.
@ Persons of Hispanic origin may be of any race.
** Includes blacks and whites of unknown ethnicity.
++ Cases reported for 1986, the first year with uniform national reporting of country of origin
for persons with tuberculosis.
&& Persons born outside the United States and its territories.
=================================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}