 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
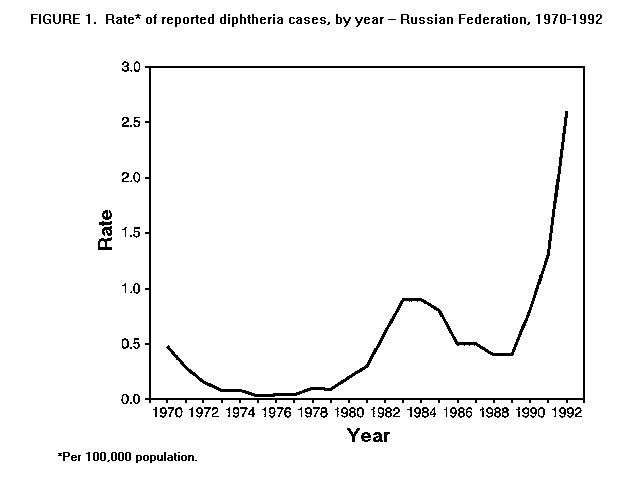
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Diphtheria Outbreak -- Russian Federation, 1990-1993Despite high levels of vaccination coverage against diphtheria, an ongoing outbreak of diphtheria has affected parts of the Russian Federation since 1990 (1); as of August 31, 1993, 12,865 cases had been reported. This report summarizes epidemiologic information about this outbreak for January 1990- August 1993, and is based on reports from public health officials in the Russian Federation. In the Russian Federation, diphtheria surveillance data are reported by physicians to the local reporting center of the Sanitary Epidemiologic Service (SES). Tabulated cases are reported to regional SESs, then forwarded to the Russian Republican Information and Analytic Center for compilation of national morbidity statistics, which are published monthly in The Health of the Population and the Environment. Diphtheria cases are investigated by local epidemiologists; case investigation forms are forwarded to the Gabrichevsky Research Institute of Epidemiology and Microbiology in Moscow for further analysis. Reported cases of diphtheria in the Russian Federation increased from 1211 (0.8 cases per 100,000 population) in 1990 to 3897 (2.6) in 1992 (Figure_1). In 1992, reported cases increased twofold over those reported in 1991; in comparison, during January- August 1993, reported cases (5888) increased threefold over those reported during the same period in 1992. In 1992, 2798 (72%) of the 3897 reported cases were among persons aged greater than 14 years; the case-fatality ratio was less than 5%. Approximately 98% of reported cases were bacteriologically confirmed. An estimated 80% of children in the Russian Federation had started their primary diphtheria-tetanus-pertussis (DTP) vaccination series* before their first birthday. However, a substantial proportion of these children received fewer than three doses by that age: during 1991, 69% of children in Moscow received one or more doses of diphtheria toxoid-containing vaccine by their first birthday; 43%, two or more doses; and 23%, three doses. However, an estimated 90% of children were fully vaccinated with four or more doses of diphtheria toxoid by the time they entered school. In 1983, the State Committee on Sanitary Epidemiologic Surveillance (SCSES) initiated a policy requiring vaccination of adults with one dose of diphtheria toxoid; however, coverage with booster doses remains low. Current efforts to control the outbreak have focused on increasing vaccination coverage among all age groups; preliminary assessment suggests that vaccine efficacy is high (Moscow SES; SCSES; CDC, unpublished data, 1993). Reported by: IN Lyetkina, NN Filatov, Moscow Sanitary Epidemiologic Service; SS Markina, Gabrichevsky Research Institute of Epidemiology and Microbiology; LG Podunova, Russian Republican Information and Analytic Center; EA Kotova, VI Chiburaev, AA Monisov, State Committee on Sanitary Epidemiologic Surveillance. National Immunization Program, CDC. Editorial NoteEditorial Note: The outbreak of diphtheria in the Russian Federation is the largest diphtheria outbreak in the developed world since the 1960s; similar levels have not been reported in the United States since the early 1950s. In addition, an outbreak of diphtheria has been reported from Ukraine, and increased diphtheria activity has been reported from many of the other New Independent States that had been members of the Soviet Union (2). The outbreak described in this report illustrates that, despite a high vaccination coverage rate among school-aged children, diphtheria can cause epidemic disease in developed countries. Strategies to control outbreaks and prevent further transmission of diphtheria include maintenance of high levels ( greater than 80%) of diphtheria vaccination coverage, ongoing surveillance, and intensive follow-up case investigation. The findings in this and previous reports underscore three important points about the epidemiology of diphtheria. First, seroprevalence studies in the United States, the Russian Federation, and other developed countries indicate that large numbers of adults remain susceptible to diphtheria (3-8). Although factors related to the occurrence of the outbreaks in the Russian Federation and Ukraine are under investigation, high levels of susceptibility to diphtheria -- particularly among adults -- have probably played an important role in sustaining transmission of infection. Second, because diphtheria remains endemic in many developing countries, these countries are a potential source for introduction of infection into developed countries. Third, the outbreak in the Russian Federation demonstrates that widespread transmission can occur in developed countries, particularly in urban areas. However, the importance of other factors (e.g., migration and crowding) also requires clarification. The risk for exposure to diphtheria cannot be readily quantified for persons who may travel to areas with endemic activity or outbreaks. Diphtheria has been reported in a visitor to the Russian Federation (9). To minimize the risk for diphtheria, the Advisory Committee on Immunization Practices recommends the following measures for all U.S. residents, especially those traveling to countries with endemic diphtheria: 1) completion of a primary series with diphtheria toxoid-containing vaccine (persons aged greater than or equal to 7 years: three doses of adult formulation tetanus-diphtheria toxoid; children aged less than 7 years: four doses of DTP vaccine {for children aged less than 7 years with a contraindication to pertussis vaccine: infant formulation diphtheria-tetanus toxoid}) and 2) receipt of the most recent dose of this vaccine (either primary series or booster dose) within the previous 10 years (10). References
* Official recommendations in the Russian Federation specify that
children should receive a dose of DTP at age 3, 4.5, and 6 months,
followed by a booster dose 1.5 2 years later; diphtheria- tetanus
toxoid boosters should be given at ages 9 and 16 years. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}