 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
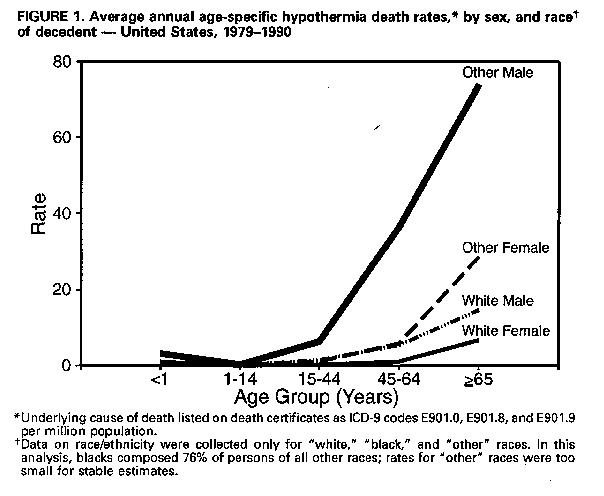
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypothermia-Related Deaths -- Cook County, Illinois, November 1992- March 1993Hypothermia results from the inability of the body to maintain a sufficiently high body temperature and is defined clinically as the lowering of core body temperature to less than or equal to 95 F (less than or equal to 35 C) (1). Environmental hypothermia results from a combination of heat loss by convection (degree of wind exposure), conduction, and radiation to the surrounding air (2). Although hypothermia-related deaths are preventable, during 1979-1990, 9362 deaths in the United States were attributed to environmental hypothermia or excessive cold (International Classification of Diseases, Ninth Revision {ICD-9}, codes E901.0, E901.8, and E901.9; excludes manmade cold {E901.1}). * From November 1992 through March 1993, 22 hypothermia-related deaths were identified by the Cook County (Chicago), Illinois (1990 population: 5,105,067), medical examiner. This report summarizes information on those deaths and describes specific findings in four of the deaths. Summary findings. Nineteen (86%) of the 22 persons who died were male, 12 (54%) were black, and six (27%) were aged greater than or equal to 65 years. Eight (36%) of the decedents were homeless. Twelve (54%) had evidence of substance abuse at autopsy examination: nine (41%), ethanol intoxication; two (9%), neuroleptic intoxication; and one (5%), narcotics. Case 1. In November 1992, a deceased 70-year-old man was found outside in a snow-covered area at the bottom of steps leading to his basement. The decedent had a history of alcohol abuse. An autopsy revealed a blood ethanol level of 0.19 g/dL. The decedent had not been seen for 36 hours before the discovery of his body, during which time outside temperatures ranged from 20 F to 35 F (- 6.7 C to 1.7 C). The underlying cause of death was hypertensive cardiovascular disease, with exposure to environmental cold secondary to alcohol intoxication being a contributing factor. Case 2. In December 1992, a deceased 45-year-old, fully clothed, homeless man was found lying on a mattress in an abandoned building. The temperature at the time he was found was 30 F (-1.1 C) with a wind chill factor of -20 F (-29.0 C). An autopsy revealed a blood ethanol level of 0.06 g/dL. Autopsy findings strongly suggested acute hemorrhagic pancreatitis, and death was attributed to acute hemorrhagic pancreatitis, with hypothermia due to cold exposure being a contributing factor. Case 3. In January 1993, police discovered a deceased 64-year-old woman who had been lying on her bed inside her unheated residence. The body was decomposed and frozen. The decedent had a history of a leg injury and limited mobility. The average low temperature for the 5 days preceding her discovery was 29 F (-1.7 C). A toxicology screen was negative; at autopsy, death was attributed to atherosclerotic cardiovascular disease, with hypothermia due to cold exposure being a contributing factor. Case 4. In March 1993, a deceased 21-year-old man was found lying on the shore of Lake Michigan; the body was lightly clothed. Autopsy findings were unremarkable, except for a blood ethanol level of 0.19 g/dL. The underlying cause of death was hypothermia, and alcohol intoxication was considered a contributing factor. Reported by: R Dames, Office of the Medical Examiner, Cook County, Chicago. Health Studies Br, and Surveillance and Programs Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC. Editorial NoteEditorial Note: Each year, approximately 780 persons in the United States die from exposure to cold **. Although these deaths are preventable, the number of deaths attributed to environmental hypothermia remained stable from 1979-1990 (annual age-adjusted death rates for hypothermia ranged from 2.2 to 4.3 per million population ***). National death rates for hypothermia during 1979-1990 varied by sex, age, and race (Figure_1). Most hypothermia-related deaths during that period occurred among men (6730 {72}%; average annual death rate: 4.9 per million population); the rate for men was 2.7 times that for women (1.8 per million population). Nearly half (4568 {49%}) of all hypothermia-related deaths occurred among persons aged greater than or equal to 65 years. Differences in hypothermia mortality by race most likely reflect differences in factors related to socioeconomic status, such as nutrition or access to adequate shelter. The age-adjusted death rate for 1979- 1990 for whites (2.4 per million population) was 3.6 times lower than the rate for persons of all other races. **** In addition, during this period the rate for white females (1.4 per million population) was 2.9 times lower than the rate for females of all other races (4.0 per million population), 2.4 times lower than the rate for white males (3.4 per million population), and 9.6 times lower than the rate for males of all other races (13.5 per million population). Persons at excess risk for hypothermia include the elderly, the very young, and the homeless, and risk factors associated with hypothermia are alcohol use, neuroleptic medications, hypothyroidism, cerebrovascular disease, some forms of mental illness, and poverty (3-5). The most common cause of hypothermia is chronic, indoor cold stress that affects the immobile, elderly, chronically ill, or poor populations (3). The elderly are particularly vulnerable because of an impaired shivering mechanism, lower levels of protective fat, lower metabolic rates, limited mobility, chronic illnesses, and lack of perception of cold (3). The onset of hypothermia is often insidious with early manifestations of exposure including shivering, numbness, fatigue, poor coordination, slurred speech, impaired mentation, blueness or puffiness of the skin, and irrationality (2,6). Measures to prevent hypothermia-related deaths include education of the public and health-care providers about heat preservation strategies and provision of outreach programs for identifying and sheltering persons at risk. During cold weather, particular attention should be given to increasing caloric intake, using insulated or layered clothing and headgear, and providing heated shelter with suitable relative humidity (3,7). In addition, persons who are active outdoors during cold weather should avoid fatigue, remain dry, prepare to take emergency shelter, carry fire-starting materials (waterproof matches and firestarters), and abstain from drinking alcoholic beverages (2,7). References
* These data were obtained from the Compressed Mortality File (CMF), provided by CDC's National Center for Health Statistics, and have been prepared in accordance with the external cause-of-death codes from the ICD-9. The CMF contains information from death certificates filed in the 50 states and the District of Columbia. ** Hypothermia-related deaths that were listed with an underlying cause of death as exposure to excessive cold (ICD-9 codes E901.0, E901.8, and E901.9 {excluding E901.1}). *** Age-adjusted death rates were standardized using the 1980 population census and are presented as deaths per million population.
**** Data on race/ethnicity were collected only for "white,"
"black," and "other" races. In this analysis, blacks composed 76%
of persons of all other races; rates for "other" races were too
small for stable estimates. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}