 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
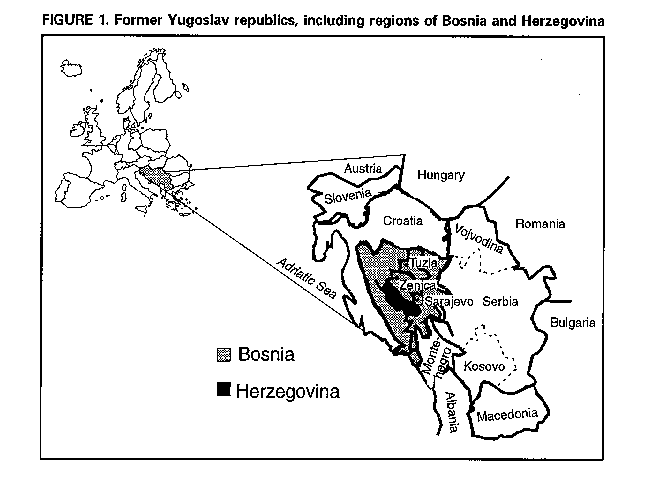
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Status of Public Health -- Bosnia and Herzegovina, August-September 1993Since 1991, civil strife in the former Yugoslav republics (Figure_1) has resulted in more than 150,000 war-related casualties (1), approximately 3.5 million displaced persons (2), widespread destruction of the health infrastructure, disruption of food production and distribution, and other increased risks to public health. The impact of the war has been especially severe in Bosnia and Herzegovina (1991 population: 4.3 million) (1). To assist in targeting humanitarian aid to the region, in August 1993, the U.S. Agency for International Development's Office of Foreign Disaster Assistance asked CDC to assess the public health status and needs of Bosnia and Herzegovina. This report summarizes the results of that assessment and focuses on three central Bosnian regions. This assessment was based on interviews with local public health officials and international humanitarian aid workers; reviews of data collected by local public health institutions and results of surveys conducted by United Nations (UN) agencies and nongovernment organizations (NGOs); and observations in central Bosnia (regions of Sarajevo, Zenica, and Tuzla) and Herzegovina. Because of security and time constraints, primary data could not be collected. The principal public health impact of the war has been injuries resulting from war-related trauma. In Sarajevo, the war accounted for more than 6800 deaths from trauma (57% of all reported mortality) and 16,000 wounded persons during April 1992- March 1993 (3). In addition, the increase in the crude mortality rate reported in Sarajevo (2.9 deaths per 1000 population in April 1993 compared with 0.8 per month in 1991) was attributed to these casualties (3). In the Zenica Provincial Hospital, the proportion of surgical cases associated with trauma increased from 22% in April 1992 (the month the war began) to a peak of 78% in December 1992 and declined to 40% in August 1993. Overall, 60% of surgical cases from July 1992 through August 1993 were war-related injuries. Based on estimates of the Office of the United Nations High Commissioner for Refugees (UNHCR), the number of persons displaced from their homes in Bosnia and Herzegovina from January 1993 through August 1993 increased from 810,000 to approximately 2 million (2). In August 1993, approximately 90% of displaced persons were living in private homes, and 10% were housed in collective centers maintained by local and international humanitarian aid agencies. Although increased numbers of displaced persons and the disruption of local agricultural production have intensified needs for international food aid, military forces representing different factions have intermittently blocked access by UN food convoys to central Bosnia. In August 1993, UNHCR was able to transport only 57% of basic food requirements for beneficiaries in the Zenica region and only 39% of requirements for the Tuzla region. Despite these limited rations, nutrition surveys conducted by the World Health Organization (WHO) in central Bosnia in July 1993 did not detect an increased prevalence of protein-energy malnutrition -- even though the mean weight loss for adults in Sarajevo since April 1992 has been 10-12 kg per person (4,5). The incidence of diagnosed cases of hepatitis A and other enteric diseases has increased in all areas of central Bosnia since the beginning of the war (Republic Institute for Public Health of Bosnia and Herzegovina, unpublished data, 1993; 6) (Table_1). The increased occurrence of enteric diseases reflects deterioration in the quantity and quality of water supplies that has resulted from diverted water sources, cracked water pipes, lack of diesel to run water pumps, and frequent losses of water pressure that, in turn, permit cross-contamination by sewage. In August 1993, for example, piped water supplies in Sarajevo were restricted to an average of 5 liters per person per day (WHO recommends daily provision of 20 liters per person to maintain health). Although some elements of the public health system continue to function, in most areas, routine prevention programs have been curtailed. For example, in central Bosnia from June 1991 through July 1993, 33% of children aged 13-25 months had been vaccinated against measles compared with coverage rates of 90%-95% in 1990 (4). However, since April 1992, no outbreaks of measles had been reported (6). In Sarajevo, during April 1992-July 1993, inadequate prenatal-care services contributed to increases in spontaneous abortions (64%) and perinatal mortality (70%) and a 19% decrease in average birthweight (S. Simic, MD, Kosevo Hospital, Sarajevo, personal communication, 1993). These prevention and other primary-care programs have been limited because of decreased access to the population, damaged health-care facilities, and inadequate supplies and resources. An especially critical supply hindered by the military blockade has been diesel, which cost $36 U.S. per gallon on the illegal market in Sarajevo in August 1993. Because of this fuel shortage, water pumps cannot function, health-care workers cannot travel to rural clinics, and some public health programs (e.g., garbage collection and vaccination campaigns) have been curtailed. Reported by: Republic Institute for Public Health of Bosnia and Herzegovina, Sarajevo, Zenica, and Tuzla. Office of the World Health Organization, Regional Office for Europe, Special Representative of the Regional Director, Zagreb, Croatia. US Office of Foreign Disaster Assistance, Washington, DC. Technical Support Div, International Health Program Office, CDC. Editorial NoteEditorial Note: During war-related emergencies in developing countries, infectious diseases consistently have been reported as the leading cause of morbidity and mortality in the affected civilian populations (7). However, the proportion of deaths in the civilian population attributed to war-related injuries in Bosnia is among the highest documented in recent humanitarian emergencies related to civil war (7). By comparison, population surveys in central and southern Somalia determined that trauma deaths accounted for 4%-11% of mortality during April 1992-January 1993 (CDC, unpublished data, 1993). Although increases in enteric disease-related mortality have not been reported, the fivefold to 16-fold increases in the incidence rates of diarrheal disease and hepatitis A from 1990 through 1993 in three central Bosnian regions underscore the urgent need for improvements in water and sanitation. Rates of infectious diseases in Bosnia are lower than those reported in civil wars in developing countries and may reflect at least five factors: 1) disease reporting has been incomplete; 2) most displaced persons are residing in private homes rather than in mass camps; 3) elements of a previously well functioning local public health system are still operating; 4) public health efforts of UN agencies and NGOs have supplemented local programs; and 5) a well educated, resourceful population has maintained relatively high standards of personal hygiene (S. Sahadzic, United Nations Children's Fund, Sarajevo, personal communication, 1993). The limited occurrence of vaccine-preventable diseases in Bosnia and Herzegovina may reflect high prewar vaccination rates and the relative absence of crowded camps that have characterized other refugee emergencies. However, measles epidemics have occurred in countries with measles vaccine coverage levels of 70% or higher (8) and the potential for such outbreaks remains high in central Bosnia. Even though the availability and distribution of food rations have been limited in Bosnia, WHO surveys suggest low prevalences of acute malnutrition. This finding may reflect a combination of four factors: 1) the presence of substantial household food reserves in 1992 (3); 2) a baseline (i.e. prewar) prevalence of elevated body mass index (9); 3) effective food distribution efforts by UNHCR from 1992 until July 1993 (2); and 4) food deliveries by commercial trucks through regular trade routes from Croatia and Serbia until April 1993 (3). This assessment was limited by the degree of underreporting and diminished sensitivity of currently operating surveillance systems. Because reports of health status provided by government sources under such circumstances may be subject to bias, independent public health surveillance and assessments should be conducted to ensure the accuracy of such reports. Priorities for relief efforts in Bosnia and Herzegovina may differ from those usually recommended for complex disasters in developing countries (7). Moreover, during 1994, the public health of residents of this region may be further threatened by lack of access by international relief agencies, limited food and fuel reserves, a likely increase in the nutritionally vulnerable population (especially children, the elderly, and pregnant women), and the severity of the winter. In addition to the identification of secure routes of access and transportation of diesel into central Bosnia, recommendations for immediate action by appropriate UN agencies and NGOs have included strengthening of programs for water and sanitation, childhood vaccination, and prenatal care and expansion of the WHO health monitoring and nutritional surveillance system. References
+-------------------------------------------------------------------
------+
| Erratum: Vol. 42, No. 50
|
|
|
| SOURCE: MMWR 43(24);450 DATE: Jun 24, 1994
|
|
|
| In the article "Status of Public Health -- Bosnia and
|
| Herzegovina, August-September 1993," the percentage change
figures |
| presented in Table 1 (Table_E1) (page 980) are incorrect. The
|
| corrected table appears below.
|
|
|
+-------------------------------------------------------------------
------+
TABLE 1. Incidence * of selected enteric diseases, by region and period -- central
Bosnia, 1990-1993
==============================================================================================
Region Hepatitis A Diarrhea Dysentery +
--------------------------------------------------------------------------
Sarajevo City &
January-June 1992 0.9 13.2 0.3
January-June 1993 5.1 94.9 4.0
% Change +560% +719% +1250%
Zenica City @
May-July 1990
and May-July 1991 0.4 10.3 0.3
May-July 1993 4.6 83.9 4.4
% Change +1210% +815% +1692%
Tuzla Region **
1992 0.5 6.5 0.5
January-June 1993 1.9 9.3 0.4
% Change +358% +43% -10.0%
--------------------------------------------------------------------------
* Per 100,000 population per month.
+ An unspecified proportion of cases were confirmed as caused by either Shigella sonnei or
S. flexneri.
& Regional Institute of Public Health, Sarajevo. Assumes a prewar population of 361,000 and
a current population of 300,000.
@ Regional Institute of Public Health, Zenica. Assumes a prewar population of 130,000 and a
current population of 195,000.
** Regional Institute of Public Health, Tuzla. Assumes a prewar and current population of
700,000.
==============================================================================================
Return to top. Figure_E1 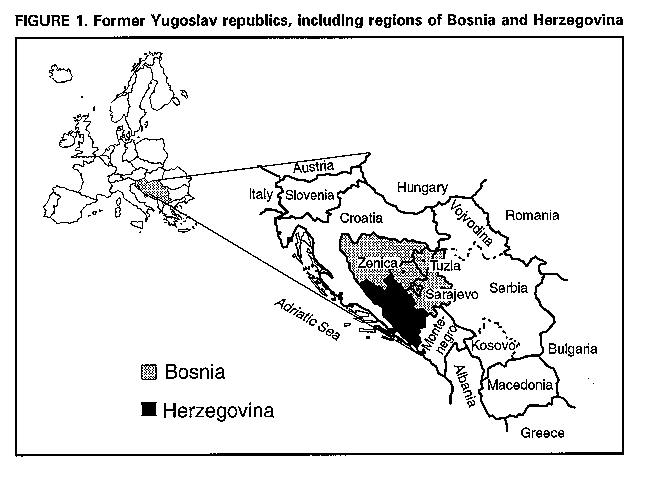 Return to top. Table_E1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Incidence * of selected enteric diseases, by region and period -- central
Bosnia, 1990-1993
==============================================================================================
Region Hepatitis A Diarrhea Dysentery +
---------------------------------------------------------------------------
Sarajevo City &
January-June 1992 0.9 13.2 0.3
January-June 1993 5.1 94.9 4.0
% Change +467% +619% +1233%
Zenica City @
May-July 1990
and May-July 1991 0.4 10.3 0.3
May-July 1993 4.6 83.9 4.4
% Change +1050% +715% +1367%
Tuzla Region **
1992 0.5 6.5 0.5
January-June 1993 1.9 9.3 0.4
% Change +280% +43% -20%
---------------------------------------------------------------------------
* Per 100,000 population per month.
+ An unspecified proportion of cases were confirmed as caused by either Shigella sonnei or
S. flexneri.
& Regional Institute of Public Health, Sarajevo. Assumes a prewar population of 361,000 and
a current population of 300,000.
@ Regional Institute of Public Health, Zenica. Assumes a prewar population of 130,000 and a
current population of 195,000.
** Regional Institute of Public Health, Tuzla. Assumes a prewar and current population of
700,000.
==============================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}