 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Primary and Secondary Syphilis -- Baltimore City, Maryland, 1995From 1993 to 1995, the number of primary and secondary syphilis cases reported in Baltimore City (1990 population: 736,014) increased 97%, from 179 to 352 cases per year (Figure_1). To identify potential reasons for this increase, CDC, in collaboration with the Baltimore City Health Department (BCHD) and the Maryland Department of Health and Mental Hygiene, analyzed data about primary and secondary syphilis cases during 1992-1995 and about temporal trends in factors that may affect syphilis rates (e.g., partner-notification results, access to medical care, and community illicit-drug use). In addition, data were analyzed from the two public sexually transmitted disease (STD) clinics in Baltimore City. BCHD collects demographic data for all cases of reported syphilis among patients who reside in Baltimore City and attempts to interview and provide partner notification and treatment for these patients. This report summarizes the results of the analysis, which suggest the outbreak has been associated with decreases in partner notification and health department clinical services and a substantial increase in community cocaine use. Epidemiology Of 344 patients with primary or secondary syphilis reported in 1995 and for whom demographic information was available, 196 (57%) were non-Hispanic black males; 120 (35%), non-Hispanic black females; 16 (5%), non-Hispanic white males; nine (3%), non-Hispanic white females; and three (1%), Hispanic (two males and one female). The mean age of males was 37.3 years (range: 13-69 years) and of females, 30.3 years (range: 14-58 years). Among persons with primary or secondary syphilis reported in 1995 and for whom self-reported sexual orientation was known, 16 (8%) of 206 men and nine (7%) of 123 women reported same-sex sexual contact since 1978; in addition, 56 (27%) men and 18 (15%) women reported exchanging money or drugs for sex. During 1995 at one of the two STD clinics, cocaine use was reported by 18 (26%) of 70 male patients with a presumptive diagnosis of primary or secondary syphilis, compared with 663 (14%) of 4780 without a presumptive diagnosis (p less than 0.01). Among female patients, cocaine use was reported by 27 (28%) of 97 with a presumptive diagnosis of primary or secondary syphilis, compared with 299 (13%) of 2281 without a presumptive diagnosis (p less than 0.01). In addition, among female patients with a presumptive diagnosis of primary or secondary syphilis, prostitution was reported by nine (35%) of 26 who reported cocaine use, compared with one (1%) of 69 who did not use cocaine (p less than 0.01). During January-September 1995, tests for human immunodeficiency virus (HIV) were positive for 22 (8%) of 265 STD clinic patients with early syphilis (i.e., primary, secondary, or early latent) who were tested for HIV at the time syphilis was diagnosed; in comparison, HIV-antibody tests were positive for 243 (3%) of 7079 STD clinic patients without early syphilis (p less than 0.01). Based on analysis of interview records, of 293 persons with early syphilis in 1995 for whom current HIV serostatus was known (including persons who were HIV-infected before their syphilis infection), 54 (18%) were HIV-infected. From 1993 to 1994, the number of clinicians at the two BCHD STD clinics decreased from 12 to eight and, from 1993 to 1995, the number of public health workers conducting partner notification decreased from 14 to eight. The contact index (i.e., the number of sex partners for whom information was sufficient to initiate efforts to locate that person divided by the number of persons with early syphilis interviewed), progressively declined from 1.3 in 1992 to 1.0 in 1995. The treatment index (i.e., the number of persons treated as a result of partner notification divided by the number of persons interviewed) declined from 0.6 in 1992 and 1.0 in 1993 to 0.4 in 1995. From 1993 to 1995, the number of self-referred patients that visited the two public STD clinics declined 12% (from 17,190 to 15,197). In comparison, during each year from 1990 through 1994, the proportion of gonorrhea cases reported from private health-care providers, a potential marker for access to private provider STD care, remained nearly constant (57% to 59%). Community Cocaine Use Based on data from the Drug Abuse Warning Network (DAWN), from 1990 through 1994, the annual number of listings of cocaine by medical examiners in drug-abuse-death cases in Baltimore City increased 737% (1) (Figure_2), and the annual number of cocaine-related emergency department episodes increased 239% (from 3023 to 10,243) (2). In addition, DAWN data indicated that the crack cocaine epidemic began in Baltimore City later than in other east coast cities. From 1990 through 1995, annual listings of crack cocaine use by Baltimore City residents entering drug treatment increased 196% (from 2131 to 6312) (Maryland Alcohol and Drug Abuse Administration, unpublished data). Reported by: P Beilenson, MD, A Garnes, MD, W Brathwaite, K West, K Becker, DVM, Baltimore City Health Dept; E Israel, MD, K Seechuk, D Dwyer, MD, State Epidemiologist, Maryland Dept of Health and Mental Hygiene. Epidemiology and Surveillance Br, Statistics and Data Management Br, Program Development and Support Br, Div of Sexually Transmitted Disease Prevention, National Center for Prevention Svcs, CDC. Editorial NoteEditorial Note: During 1990, the rate for primary and secondary syphilis in the United States (20.3 per 100,000 population) was the highest since the 1940s and approximately 10-fold higher than in other industrialized countries (3). Use of crack cocaine and the exchange of sex for drugs were identified as major contributors to this epidemic (4). Although the national rate had declined to 8.1 by 1994, endemic disease at high rates persists in some communities and outbreaks continue to occur. The investigation of primary and secondary syphilis in Baltimore City identified epidemiologic patterns consistent with other urban areas of the United States: most cases occurred among blacks, and cocaine use and the exchange of money or drugs for sex were frequently reported risk behaviors; the predominance of cases among blacks may reflect factors including area of residence, socioeconomic status, and access to health services. A communitywide expansion in crack cocaine use preceded the increase in Baltimore City and most likely was the primary contributing factor. In addition, a decline in clinical and partner-notification service staffing may have limited the public health response to the increase in cases, although cocaine-associated syphilis outbreaks may be characterized by lower partner notification indices independent of available personnel (5). At least three potential intersecting epidemics may be associated with the increased occurrence of early syphilis in Baltimore City, including crack-cocaine use, congenital syphilis, and HIV infection. Because the numbers of syphilis-infected pregnant women in Baltimore City may increase, efforts to prevent congenital syphilis must be intensified (6). HIV transmission in Baltimore City may be increasing because HIV infection is associated with the use of crack cocaine (7) and because genital ulcers directly facilitate HIV transmission (8). In a previous syphilis epidemic, 18% of all documented HIV seroconversion in STD clinic patients was attributable to syphilis infection (9). Because of the duration of the incubation period of HIV and its effect on recognition of HIV transmission patterns, additional efforts should assess whether early syphilis rates are useful indicators of risk for HIV transmission. To control the increase in syphilis cases, BCHD is alerting the medical community about the syphilis outbreak (e.g., letters to and teleconferences with health-care providers), filling STD program personnel vacancies, and expanding case-finding and surveillance activities. References
Figure_1 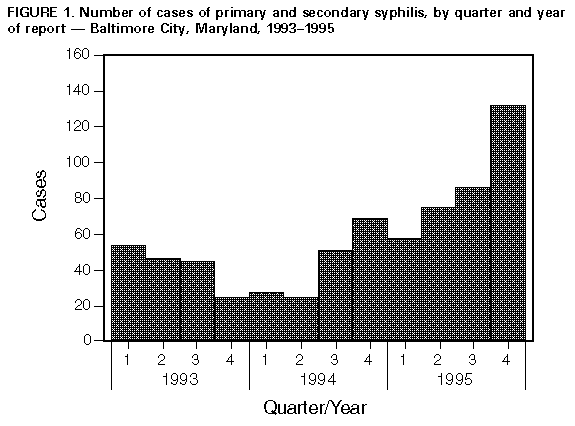 Return to top. Figure_2 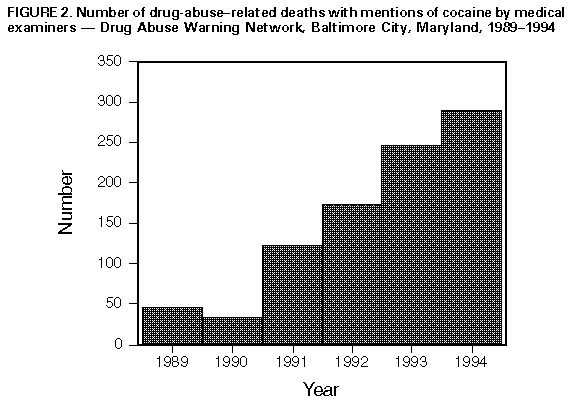 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}