 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Morbidity -- United States, 1995During 1995, a total of 22,813 cases of tuberculosis (TB) (8.7 cases per 100,000 population) were reported to CDC from the 50 states, the District of Columbia (DC), and New York City -- a 6.4% decrease from 1994 (24,361 cases {9.4 per 100,000}) (1); an additional 262 cases were reported from Puerto Rico. This represents the third consecutive year the number of reported TB cases has decreased (Table_1) (2), resulting in the lowest rate for reported TB cases since national surveillance began in 1953. This report summarizes TB surveillance data for 1995 and compares these data with selected data for 1986-1994, and indicates a decreased number of TB cases among U.S.-born persons and increased number among foreign-born persons. During 1995, a total of 32 states and DC reported fewer TB cases than in 1994; in comparison, during 1994, a total of 26 states and DC reported fewer cases than in 1993, and during 1993, a total of 31 states reported fewer cases than in 1992 (Table_1). Nine states (California, Connecticut, Hawaii, Illinois, Michigan, Mississippi, New Jersey, New York, and North Carolina) reported fewer cases each year since 1992, a total of 18 states (36%) reported no change or more cases in 1995 compared with 1994, and two (Iowa and Kansas) reported more cases in each year since 1992 (Table_1). Compared with 1994, the number of reported TB cases in 1995 decreased in each sex and age group and all racial/ethnic groups except Asians/Pacific Islanders, for whom a 2.9% increase was reported (Table_2). During 1995, TB cases reported among persons born outside the United States and its territories (i.e., foreign-born) accounted for 35.7% of total reported cases, compared with 31.3% in 1994 (Table_2). The number and proportion of persons reported with TB who were classified as foreign-born have increased 63.3% since 1986, the first year information on the country of origin was collected for each case (Figure_1). In 1995, the country of origin was known for 7592 (94.4%) cases reported in foreign-born persons; six countries (Haiti, India, Mexico, People's Republic of China, Philippines, and Vietnam) accounted for 63.6% of the cases. Of the 4804 foreign-born persons reported in 1995 whose records contained information about month and year of arrival in the United States, 1441 (30.0%) had TB diagnosed within 1 year and 2567 (53.4%) within 5 years after entering the United States. Compared with 1994, the number of cases reported in U.S.-born persons in 1995 decreased 10.8%, and the number of cases in foreign-born persons increased 5.4% (Table_2). During 1995, the number of cases in U.S.-born persons decreased in all age groups; the decrease was largest (17.0%) among persons aged 25-44 years. In comparison, the number of cases in foreign-born persons reported in 1995 increased in all age groups except for children aged less than 15 years (decreased 7.4%) and persons aged 15-24 years (decreased 5.1%). Human immunodeficiency virus (HIV)-antibody test results were available in 1994 for 3317 (36.4%) of 9106 patients aged 25-44 years (nine states reported this information for greater than or equal to 75% of records) and in 1995 for 2925 (35.6%) of 8227 such patients (eight states reported information for greater than or equal to 75% of records). Information about the prescribed initial drug regimen for each TB case was available for 98.0% of cases reported in both 1994 and 1995. Compared with 1994, in 1995 there was a 5.3% increase in the proportion of cases for which the initial four-drug regimen was prescribed as recommended by the Advisory Council for the Elimination of Tuberculosis, the American Thoracic Society, and CDC (isoniazid {INH}, rifampin {RIF}, pyrazinamide {PZA}, and either ethambutol or streptomycin) (3,4) (Table_2). The proportion of patients for whom drug-susceptibility results for Mycobacterium tuberculosis isolates were reported was larger in 1995 than in 1994 (14,052 {77.3%} of 18,168 patients and 14,509 {74.3%} of 19,537 patients, respectively). In 1995, a total of 37 states reported drug-susceptibility results for isolates from greater than or equal to 75% of cases; of these, 806 (7.6%) of 10,621 isolates were resistant to at least INH, and 145 (1.4%) of 10,611 were resistant to at least INH and RIF. Compared with 1994, when only 23 states reported drug-susceptibility results for isolates from greater than or equal to 75% of cases, the proportion of cases with isolates resistant to at least INH decreased from 8.5%, and resistance to at least INH and RIF decreased from 1.5%. The 37 states reporting drug-susceptibility results accounted for 71% of all culture-positive cases reported in the United States in 1995. Reported by: Div of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention (proposed), CDC. Editorial NoteEditorial Note: The substantial decline in the number of TB cases reported annually in the United States during 1992-1995 (14.5%) reflects at least six factors: 1) improved laboratory methods to allow prompt identification of M. tuberculosis; 2) broader use of drug-susceptibility testing; 3) expanded use of preventive therapy in high-risk groups; 4) decreased transmission of M. tuberculosis in congregative settings (e.g., hospitals and correctional facilities) by implementing infection-control guidelines (5,6); 5) improved follow-up of persons with TB initially reported to the health department, leading to subsequent removal from the surveillance database of cases for which a disease other than TB was diagnosed; and 6) increased federal resources for state and local TB-control efforts. Beginning in 1992, federal resources for assisting state and local TB-control efforts were increased (1,7). Some of the states with the largest decreases (e.g., New York and California) had high rates of HIV infection and acquired immunodeficiency syndrome (AIDS); resources directed to these states also have supported TB-screening efforts and preventive therapy for HIV-infected persons at high risk for TB infection. The increased funding enabled state and local TB-control programs to improve management of TB cases, in part by ensuring that all patients complete an adequate course of therapy and by expanding the use of directly observed therapy (7,8). Preliminary analyses of national surveillance data and TB-control program management reports indicate that the decrease in cases in U.S.-born persons largely reflected improvement in program performance (CDC, unpublished data, 1995). Since 1986, the number and proportion of reported TB cases among foreign-born persons have increased substantially (9). Most of these persons develop TB disease within the first 5 years of arrival in the United States because of reactivation of latent M. tuberculosis infection acquired in their country of origin, inadequate screening for and/or treatment of TB before entering the United States, or inadequate follow-up of those who have entered the United States with noninfectious TB (i.e., abnormal chest radiograph with negative sputum smears). Control of TB among foreign-born persons in the United States can be strengthened through improved screening and services for immigrants and refugees, prompt reporting of immigrants and refugees with suspected TB to public health programs and health-care providers, and early identification and treatment of TB in foreign-born persons from countries with a high prevalence of TB (9). Assessment of the relation between HIV infection and TB has been limited by the incomplete reporting of information on HIV test results for TB cases: during 1994-1995, this information was available for only 36% of reported persons aged 25-44 years. During 1996 and 1997, CDC, in collaboration with selected state and local health departments, will assess HIV-testing and HIV-counseling practices for TB patients, measure the prevalence of testing, and determine barriers to reporting HIV results for patients who are tested. Results of this assessment will be used to develop strategies to improve HIV testing and counseling of TB patients and reporting of HIV results to state and local TB and HIV/AIDS surveillance programs. The recent national decreases in TB morbidity in the United States can be sustained through efforts by federal agencies and state and local health departments to ensure that all persons with TB are promptly identified and treated. These efforts especially must include the identification and treatment of cases in foreign-born persons and persons who are HIV infected. In addition, TB skin tests of high-risk persons will enable identification of persons who could benefit from preventive therapy. References
Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Number of reported tuberculosis cases and percentage change, by state and
year -- United States, 1992-1995
=================================================================================================
No. cases % Change
------------------------------------- ----------------------------------
State 1992 1993 1994 1995 1992-1993 1993-1994 1994-1995
-----------------------------------------------------------------------------------------------
Alabama 418 487 433 420 +16.5 -11.1 - 3.0
Alaska 57 57 93 81 0 +63.2 -12.9
Arizona 259 231 249 319 -10.8 + 7.8 +28.1
Arkansas 257 209 264 271 -18.7 +26.3 + 2.7
California 5,382 5,170 4,859 4,622 - 3.9 - 6.0 - 4.9
Colorado 104 104 94 95 0 - 9.6 + 1.1
Connecticut 156 155 148 140 - 0.6 - 4.5 - 5.4
Delaware 55 66 57 56 +20.0 -13.6 - 1.8
District of
Columbia 146 161 121 102 +10.3 -24.8 -15.7
Florida 1,707 1,655 1,762 1,557 - 3.0 + 6.5 -11.6
Georgia 893 812 740 746 - 9.1 - 8.9 + 0.8
Hawaii 273 251 247 193 - 8.1 - 1.6 -21.9
Idaho 26 11 13 14 -57.7 +18.2 + 7.7
Illinois 1,270 1,237 1,117 1,024 - 2.6 - 9.7 - 8.3
Indiana 247 248 211 199 + 0.4 -14.9 - 5.7
Iowa 49 59 66 72 +20.4 +11.8 + 9.1
Kansas 56 80 84 89 +42.9 + 5.0 + 6.0
Kentucky 402 404 347 327 + 0.5 -14.1 - 5.8
Louisiana 373 367 433 476 - 1.6 +18.0 + 9.9
Maine 24 28 35 28 +16.7 +25.0 -20.0
Maryland 442 417 363 370 - 5.7 -13.0 + 1.9
Massachusetts 428 370 329 330 -13.6 -11.1 + 0.3
Michigan 495 480 462 424 - 3.0 - 3.8 - 8.2
Minnesota 165 144 140 156 -12.7 - 2.8 +11.4
Mississippi 281 279 278 271 - 0.7 - 0.4 - 2.5
Missouri 245 257 260 245 + 4.9 + 1.2 - 5.8
Montana 16 22 24 21 +37.5 + 9.1 -12.5
Nebraska 28 23 22 24 -17.9 - 4.4 + 9.1
Nevada 99 99 126 115 0 +27.3 - 8.7
New Hampshire 18 26 17 23 +44.4 -34.6 +35.3
New Jersey 984 912 855 848 - 7.3 - 6.3 - 0.8
New Mexico 88 74 81 84 -15.9 + 9.5 + 3.7
New York* 4,574 3,953 3,636 3,066 -13.6 - 8.0 -15.7
North Carolina 604 594 566 519 - 1.7 - 4.7 - 8.3
North Dakota 11 7 10 5 -36.4 +42.9 -50.0
Ohio 358 315 337 280 -12.0 + 7.0 -16.9
Oklahoma 216 209 261 237 - 3.2 +24.9 - 9.2
Oregon 145 154 165 156 + 6.2 + 7.1 - 5.5
Pennsylvania 758 749 621 680 - 1.2 -17.1 + 9.5
Rhode Island 54 64 56 50 +18.5 -12.5 -10.7
South Carolina 387 401 387 334 + 3.6 - 3.5 -13.7
South Dakota 32 16 28 28 -50.0 +75.0 0
Tennessee 527 556 520 465 + 5.5 - 6.5 -10.6
Texas 2,510 2,396 2,542 2,369 - 4.5 + 6.1 - 6.8
Utah 78 46 55 48 -41.0 +19.6 -12.7
Vermont 7 7 10 4 0 +42.9 -60.0
Virginia 457 458 372 359 + 0.2 -18.8 - 3.5
Washington 306 285 264 278 - 6.9 - 7.4 + 5.3
West Virginia 92 75 80 71 -18.5 + 6.7 -11.3
Wisconsin 106 100 109 117 - 5.7 + 9.0 + 7.3
Wyoming 8 7 12 5 -12.5 +71.4 -58.3
Total 26,673 25,287 24,361 22,813 - 5.2 - 3.7 - 6.4
-----------------------------------------------------------------------------------------------
*Includes New York City.
=================================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Number of persons with reported cases of tuberculosis, by selected
characteristics and year -- United States, 1994-1995
======================================================================================
No. reported cases
-------------------- % Change,
Characteristic 1994 1995 1994-1995
----------------------------------------------------------------------------
Sex *
Male 15,833 14,482 - 8.5
Female 8,517 8,301 - 4.9
Age group (yrs) +
0-14 1,695 1,551 - 8.5
15-24 1,825 1,700 - 6.9
25-44 9,106 8,227 - 9.7
45-64 6,141 5,985 - 2.5
>=65 5,546 5,332 - 3.9
Race/Ethnicity &
White, non-Hispanic 6,494 5,950
Black, non-Hispanic 8,345 7,521
Hispanic 5,074 4,808 - 5.2
Asian/Pacific Islander 3,821 3,932 + 2.9
American Indian/
Alaskan Native 332 323 - 2.7
Country of origin @
United States 16,278 14,515 -10.8
Other 7,627 8,042 + 5.4
Initial drug regimen **
Isoniazid and rifampin 1,626 1,083 -33.4
Isoniazid, rifampin, and
pyrazinamide 5,332 4,325 -18.9
Isoniazid, rifampin,
pyrazinamide, and ethambutol
or streptomycin 12,768 13,439 + 5.3
Other 3,019 2,373 -21.4
Total 24,361 22,813 - 6.4
----------------------------------------------------------------------------
* Excludes persons for whom sex was unknown (11 in 1994 and 30 in 1995).
+ Excludes persons with unknown or missing age (48 in 1994 and 18 in 1995).
& Excludes persons with unknown race/ethnicity (295 in 1994 and 279 in 1995).
@ Excludes persons with unknown country of origin (456 in 1994 and 256 in 1995).
** Excludes persons with unknown or no drug regimen (1616 in 1994 and 1593 in 1995).
======================================================================================
Return to top. Figure_1 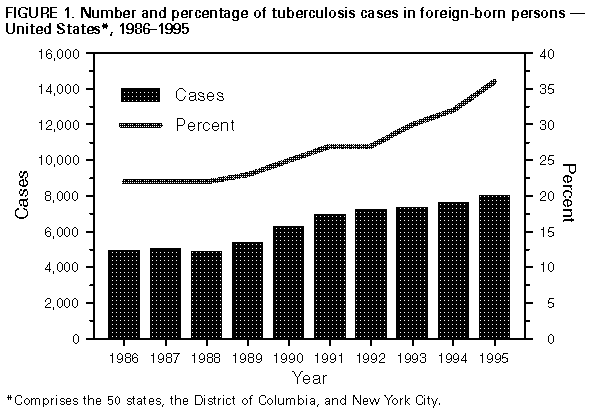 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}