 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
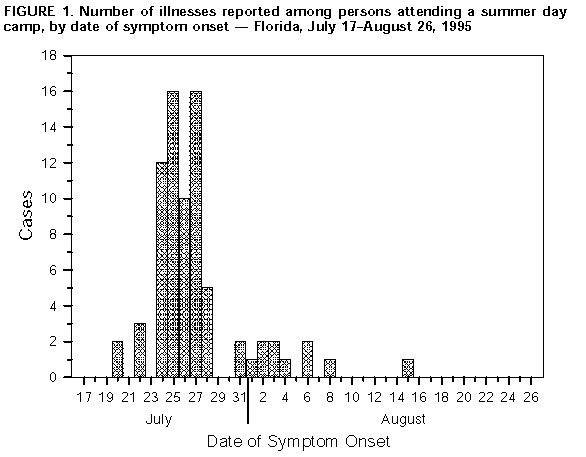
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Cryptosporidiosis at a Day Camp -- Florida, July-August 1995On July 27, 1995, the Alachua County Public Health Unit (ACPHU) in central Florida was notified of an outbreak of gastroenteritis among children and counselors at a day camp on the grounds of a public elementary school. This report summarizes the outbreak investigation, which implicated Cryptosporidium parvum as the causative agent and underscores the role of contaminated water as a vehicle for transmission of this organism. The camp operated from June 12 through August 4 and enrolled 98 children (age range: 4-12 years) and six counselors during the 3 weeks before the outbreak. A confirmed case of cryptosporidiosis was defined as gastrointestinal symptoms (i.e., abdominal pain, nausea, vomiting, and three or more watery stools each day) in a camp attendee during July 20-August 23 with C. parvum isolated in stool. A probable case was defined as gastrointestinal symptoms during July 20-August 23 in a camp attendee who did not submit a stool sample for testing. A questionnaire was administered to each of the 104 persons attending the camp; for some children, information was obtained from parents and camp records. Of the 104 persons attending the camp, 77 (74%) had symptoms (abdominal pain {74%}, nausea {73%}, diarrhea {71%}, vomiting {57%}, and fever {43%}) with onset during July 20-August 15, including 72 of 98 children and five of six counselors (Figure_1). Follow-up phone calls to 67 of 79 households of those who attended the camp indicated that 24 household members had onset of gastrointestinal symptoms during July 20-August 23. Stool specimens for bacterial enteric pathogen testing were obtained from 44 camp attendees within 10 days of onset of symptoms; all were negative. Sixteen stool specimens were obtained for testing for ova and parasites; all 16 yielded C. parvum. Risk for illness was not associated with participating in a particular camp activity or eating a lunch or snack provided by the camp. Water sources for the camp included an outdoor drinking fountain, a sink inside the trailer that served as camp headquarters, and portable coolers. The coolers were filled at either a kitchen sink inside the school or an outdoor faucet with an attached hose and spray nozzle used for washing garbage cans. Although water consumption from any source could not be quantified, virtually all persons at the camp reported drinking water from one of the camp sources during the 3 weeks before the outbreak. Water samples were tested (1) from the city's water treatment plant, all school sources used by campers, and three sinks inside the school. The water treatment plant samples were repeatedly negative. Outdoor faucet samples were positive for total coliforms and C. parvum; other tests from school sites were negative or below detectable limits for total coliform, Escherichia coli, and ova and parasites. The area around the outdoor faucet was not fenced, and feces of unknown origin were observed on several occasions near the faucet and attached hose. Based on these findings, ACPHU recommended discontinuing use of coolers for water and the outdoor faucet, and enclosing the faucet area by fence. In addition, parents and staff were taught proper handwashing technique and given information about C. parvum. Staff returning to school used alternate water sources until the system was superchlorinated, flushed, and cleared. Reported by: J Regan, R McVay, M McEvoy, J Gilbert, Water and Wastewater Systems, Gainesville Regional Utilities. R Hughes, T Tougaw, E Parker, PhD, W Crawford, J Johnson, School Board of Alachua County, Gainesville, Florida. J Rose, PhD, Univ of South Florida, St. Petersburg, Florida. S Boutros, PhD, Environmental Associates Ltd, Bradford, Pennsylvania. S Roush, MPH, T Belcuore, MS, C Rains, MD, J Munden, MPH, Alachua County Public Health Unit; L Stark, PhD, E Hartwig, ScD, M Pawlowicz, Florida Dept of Health and Rehabilitative Svcs State Laboratory; R Hammond, PhD, D Windham, R Hopkins, MD, State Epidemiologist, Florida Dept of Health and Rehabilitative Svcs. Div of Field Epidemiology, Epidemiology Program Office, CDC. Editorial NoteEditorial Note: The protozoan parasite C. parvum was first identified as a human pathogen in 1976; since then, the organism has been increasingly recognized as an agent of gastrointestinal illness. In immunocompetent persons, cryptosporidiosis can cause moderately severe watery diarrhea that usually lasts 1-20 days (average: 10 days) (2). In immunocompromised persons (e.g., those with acquired immunodeficiency syndrome {AIDS} or those taking certain chemotherapeutic regimens), the infection can cause severe, unrelenting diarrhea. The antibiotic paromomycin can improve symptoms and decrease parasite excretion in the feces of some persons with AIDS and is the treatment of choice for immunosupppressed patients (3,4). Cryptosporidiosis is transmitted by the fecal-oral route, most commonly by direct person-to-person transmission or by drinking water that has been contaminated with human or animal feces. In 1993, cryptosporidiosis caused the largest waterborne disease outbreak ever recorded, when an estimated 400,000 persons in Milwaukee became ill after drinking contaminated municipal water (5). The outbreak described in this report most likely was related to drinking contaminated water. Contamination probably occurred at the nozzle of the hose used to fill the water coolers rather than at or near the water treatment plant. Sources of drinking water should be protected from possible fecal contamination, and hoses, which are particularly susceptible to back-syphonage, should not be used to provide drinking water. Public water sources that cannot be protected should be posted as nonpotable. C. parvum was promptly identified as the source of this outbreak, in part because the Florida State Public Health Laboratory examines all fecal specimens submitted for ova and parasite analysis for C. parvum. The diagnosis of cryptosporidiosis can be delayed or missed when physicians assume incorrectly that diagnostic laboratories routinely perform specific tests for C. parvum when a fecal examination for parasites is requested. A recent national survey of clinical laboratories found that only 5% did so (6). If cryptosporidiosis is suspected in the differential diagnosis, physicians should specifically request testing for C. parvum. In addition, when reporting the results of fecal examinations, clinical laboratories should specify what tests were performed rather than only indicating that no enteric pathogens were identified. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}