 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
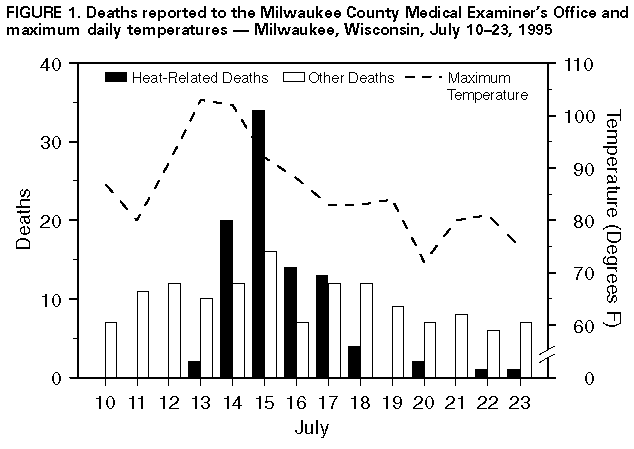
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Heat-Wave-Related Mortality -- Milwaukee, Wisconsin, July 1995During July 12-15, 1995, a heat wave * occurred in major portions of the midwestern and eastern United States. Record-high temperatures were recorded at approximately 70 locations, ranging from the central and northern Great Plains to the Atlantic coast (1) and caused substantial numbers of heat-related illnesses and deaths in some locations (2). In Milwaukee, Wisconsin (1994 estimated population: 938,112), maximum daily temperatures ranged from 91 F (32.7 C) to 103 F (39.5 C), and average daily humidity was as high as 70%. This report summarizes the investigation by the Milwaukee County Medical Examiner's Office (MCMEO) and the Milwaukee Department of Health and Social Services of heat-related deaths in Milwaukee during the heat wave and presents four case reports. Investigation of Deaths During July 13-23, MCMEO received reports of and investigated 197 deaths. Of these, 91 (46%) were determined to be related to the heat wave. Deaths were considered heat-related if 1) the decedent's measured body temperature at the time of death was greater than or equal to 105 F (greater than or equal to 40.4 C), or 2) there was evidence of high environmental temperature -- usually greater than or equal to 100 F (greater than or equal to 37.7 C) -- at the scene of death. Hyperthermia or excessive heat was cited as the underlying or direct cause for 34 (37%) of these 91 deaths and as an important contributing cause for 57 (63%). The 91 decedents ranged in age from 1 year to 97 years (median: 76 years), and 52 (57%) were male. Psychotropic medications were cited as contributing factors in 15 deaths, and alcohol consumption was cited as a contributing factor in five. Eighty-one (89%) of the deaths occurred during July 14-17, and 34 (42%) of these occurred on July 15 (Figure_1). Case Reports Case 1. On July 13, 1995, a 7-month-old girl was brought to an emergency department because of respiratory arrest but could not be resuscitated. The cause of death was listed by MCMEO as bronchopulmonary dysplasia associated with environmental hyperthermia. She had been receiving home nursing care for congenital respiratory impairment. A window air conditioner was being installed at the time of her death. Case 2. On July 14, 1995, an 82-year-old woman was found dead in her two-story home. A neighbor reported that the decedent had had no health complaints the previous evening. Family members reported that the decedent had used a fan but kept all doors and windows closed because of safety concerns; the wall thermostat registered greater than 90 F (greater than 32.2 C) on the day before death. The immediate cause of death was listed by MCMEO as arteriosclerotic heart disease, with elevated environmental temperature as an important contributing factor. Case 3. On July 15, 1995, a 24-year-old man with a history of schizophrenia, acute depression, and psychotropic drug use was found dead in the living room of his family residence. The previous day he had reported "not feeling well." The immediate cause of death was listed by MCMEO as environmental hyperthermia, with use of psychotropic medications as an important contributing factor. Case 4. On July 17, 1995, a 79-year-old woman was found dead in her home. She had last been seen returning from a store on the previous day by a neighbor. The immediate cause of death was listed by MCMEO as arteriosclerotic heart disease, with elevated environmental temperature as an important contributing factor. Reported by: R Nashold, PhD, P Remington, MD, P Peterson, Center for Health Statistics and Registrar of Vital Statistics, Div of Health, Wisconsin Dept of Health and Social Svcs; J Jentzen, MD, Milwaukee County Medical Examiner's Office, Milwaukee, Wisconsin. R Kapella, National Weather Service, Champaign, Illinois. Health Studies Br and Surveillance and Programs Br, Div of Enivironmental Hazards and Health Effects, National Center for Environmental Health, CDC. Editorial NoteEditorial Note: During periods of sustained environmental heat -- particularly during the summer -- the numbers of deaths classified as heat-related (e.g., heatstroke) and attributed to other causes (e.g., cardiovascular, cerebrovascular, and respiratory disease) increase substantially (3). The epidemiology of the heat-related deaths in Milwaukee in 1995 is consistent with previous reports indicating increased risk for heat-related mortality among elderly persons, persons with chronic conditions (including obesity), patients taking medications that predispose them to heatstroke (e.g., neuroleptics or anticholinergics), and persons confined to bed or who otherwise are unable to care for themselves (4,5). Adverse health outcomes associated with high environmental temperatures include heatstroke, heat exhaustion, heat syncope, and heat cramps (6). Heatstroke (i.e., core body temperature greater than or equal to 105 F (greater than or equal to 40.4 C) is the most serious of these conditions and is characterized by rapid progression of lethargy, confusion, and unconsciousness; it is often fatal despite medical care directed at lowering body temperature. Heat exhaustion is a milder syndrome that occurs following sustained exposure to hot temperatures and results from dehydration and electrolyte imbalance; manifestations include dizziness, weakness, or fatigue, and treatment is supportive. Heat syncope and heat cramps usually are related to physical exertion during hot weather; persons with loss of consciousness resulting from heat syncope should be treated by placement in a recumbent position and replacement of electrolytes. Basic behavioral and environmental measures are essential for preventing heat-related illness and death. Personal prevention strategies should include increases in time spent in air-conditioned environments, intake of nonalcoholic beverages, and incorporation of cool baths into a daily routine. When possible, activity requiring physical exertion should be conducted during cooler parts of the day. Sun exposure should be minimized, and light, loose, cotton clothing should be worn. The risk for heat-induced illness is greatest before persons become acclimatized to warm environments. Athletes and workers in occupations requiring exposure to either indoor or outdoor high temperatures should take special precautions, including allowing 10-14 days to acclimate to an environment of predictably high ambient temperature. Public health agencies can assist in preventing heat-related illnesses and deaths by disseminating community prevention messages to persons at high risk (e.g., the elderly and persons with preexisting medical conditions) using a variety of communication techniques and establishing emergency plans that include provision of access to artificially cooled environments. References
Three or more consecutive days of air temperatures greater than
90 F
(greater than 32.2 C). Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}