 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
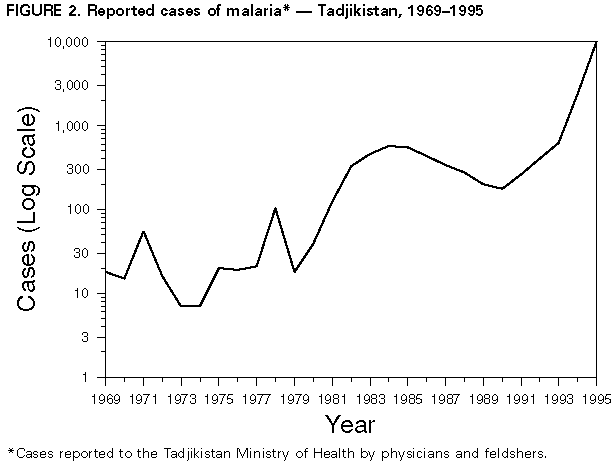
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Epidemic Malaria -- Tadjikistan, 1995In June 1995, the Tadjikistan Ministry of Health (MOH) and CDC, with support of the U.S. Agency for International Development, began collaborative efforts to strengthen the health information and disease surveillance systems in Tadjikistan (1995 population: 5.7 million) (Figure_1). As part of an initial evaluation in Tadjikistan, the Republican Sanitary and Epidemiologic Service (RSES) and the Parasitology Laboratory of the Institute for Preventive Medicine in the MOH reported a substantial increase in the incidence of malaria since 1991. This report summarizes malaria surveillance data for 1995 in Tadjikistan and describes barriers to implementing effective measures for controlling and preventing malaria in Tadjikistan. The MOH requires reporting of all malaria cases; reporting sources include physicians and feldshers (health-care workers similar to physician's assistants who often are the first contact patients may have with the medical system, especially in rural areas) who examine patients in hospitals, polyclinics, diagnostic centers, ambulatory clinics, or individual feldsher stations. All cases of malaria -- whether confirmed or suspected -- must be reported to the MOH within 12 hours. Each case is reviewed, and an investigation may be initiated to examine the diagnosis, exposure, and treatment. Cases enumerated in the surveillance system are those with a final diagnosis of malaria, based on the clinician's evaluation and/or results of the investigation, and may not require laboratory confirmation. Historically, reported malaria data in Tadjikistan were assessed for validity through a systematic random-sample surveillance system requiring that a blood slide of every 10th smear-confirmed case be sent to the RSES for confirmation; the RSES then sent the slides to the Institute of Preventive Medicine for additional confirmation. The system also required that a blood slide of every 10th smear performed for initially suspected cases that were investigated but not confirmed be sent to the Sanitary and Epidemiologic Service at the oblast (state) level for examination. During the fourth quarter of 1995, this system was unreliable because of shortages of trained personnel. During the 1960s and 1970s, sporadic cases of infection with Plasmodium vivax occurred in persons in Tadjikistan who resided in the area of the Amu Darya River basin that separates Tadjikistan from Afghanistan; from 1972 through 1978, annual case counts were consistently less than or equal to 21 (Figure_2). Malaria transmission in Tadjikistan was limited by mosquito-eradication efforts that included aerial spraying with insecticides. Following the start of the war in Afghanistan in 1979, the number of reported cases in Tadjikistan increased sharply, peaking at 571 cases (12.7 per 100,000 population) in 1984, reflecting in part disruption of intensive efforts for mosquito control in both Tadjikistan and Afghanistan. Mosquito-control activities were resumed in the mid-1980s, and the total number of reported malaria cases in Tadjikistan had declined to 176 in 1990. Mosquito-control operations were curtailed in 1991 because of financial constraints and discontinued in 1992. Beginning in 1991, the annual number of confirmed cases of malaria increased dramatically (Figure_2). The 619 cases of malaria reported in 1993 included the first reported cases of P. malariae and P. falciparum. In 1994, of the 2411 total cases of malaria, 54 (2.2%) were identified as P. falciparum; the remainder were identified as P. vivax or P. malariae infection. The overall incidence of malaria in 1994 was 43.4 per 100,000 population. Of the 2411 total cases, 1638 (70.7%) were reported from Hatlon Oblast (86.7 per 100,000), and 446 (18.5%) were reported from the Gorno-Badakhshan Autonomous Region (227.3 per 100,000). Of the cases reported from Hatlon Oblast, the incidence was highest in those districts bordering Afghanistan. In addition, in at least three administrative districts with populations of approximately 30,000 each, the incidence was greater than or equal to 300 per 100,000. During January-September 1995, a total of 4332 cases of malaria were reported, a 146% increase over the same period in 1994 (1764 cases). Although the final total number of new malaria cases in Tadjikistan in 1995 is unknown, an estimated 10,000 cases occurred, based on historical ratios of initial reports to confirmed cases; however, few of these new cases were slide-confirmed. In addition, during January-September 1995, 470 cases were reported in the capital city of Dushanbe (88.2 per 100,000). Although most of these cases occurred among persons who probably acquired infection in the southern oblasts bordering Afghanistan, approximately 24% did not have confirmed recent travel histories to a malaria-endemic area and may have acquired infection locally or these cases may represent relapses. More detailed epidemiologic description of cases (e.g., age and sex) and an accurate number of malaria-related deaths are not available. Chloroquine resistance has not been reported, although detailed drug-sensitivity studies have not been conducted. Reported by: B Shoismatullaev, Republican Sanitary and Epidemiologic Service; A Sharipov, Kurgan-Tyube Zone Sanitary and Epidemiologic Svc; A Umarova, N Elizarova, F Odinaev, Institute of Preventive Medicine; and I Usmanov, Central Offices, Tadjikistan Ministry of Health. International Health Program Office; Malaria Section, Epidemiology Br, Div of Parasitic Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: An estimated 40% of the world's population is at risk for malaria infection; each year, 300-500 million clinical cases and 1.5-2.7 million malaria-associated deaths occur (1). Important components of the Global Malaria Control Strategy described by the World Health Organization (WHO) are recognition of areas at risk for outbreaks of malaria and epidemic preparedness (2). Factors associated with the increased risk for epidemic malaria in Tadjikistan include the large population movements near the Afghanistan border, adverse economic conditions, breakdown of health-care services, shortages of trained public health personnel, and ongoing civil war that has constrained epidemiologic investigation and implementation of control activities (3). Systematic preventive measures -- including mosquito control -- have been suspended because of shortages of gasoline, equipment, and insecticides. Production of crops that require irrigation in an arid area (e.g., rice and corn) also is increasing, resulting in an increase in suitable anopheline breeding sites and possibly contributing to the increase in malaria transmission. Since the government of Tadjikistan declared independence in September 1991, political unrest and a decline in economic conditions have resulted in an exodus of trained epidemiologists and support personnel to other countries. Of 200 trained epidemiologists in the Tadjikistan RSES before independence, less than 25 remain. Underreporting also is increasing as persons are less likely to seek health-care services. In addition, although WHO has provided large quantities of antimalarials, only 50%-70% of cases have received optimal treatment with chloroquine and primaquine to treat the blood-stage parasites and to prevent relapses of P. vivax infection. Infection with P. falciparum in a population with no prior exposure could cause severe illness with high case-fatality rates among both children and adults. Because many cases in Tadjikistan were imported among refugees returning from northern Afghanistan, an area with chloroquine-resistant P. falciparum, surveillance for drug resistance especially is important for development of treatment protocols. Malaria transmission in Tadjikistan occurs primarily from the end of May through November. Because of the potential for intensification of the malaria epidemic, the surveillance system needs to be strengthened and include collection of travel and exposure history to help target control measures. Optimal case management will require rebuilding diagnostic capability, ensuring ample supplies of antimalarial drugs, and having standardized treatment protocols. Improving the ability to monitor anopheline populations will focus control measures and target the use of insecticides and aerial and house spraying. A needs assessment will be necessary to assist in developing enhanced surveillance, improved case management, and vector control, and to guide assistance from the international donor community. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}