 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
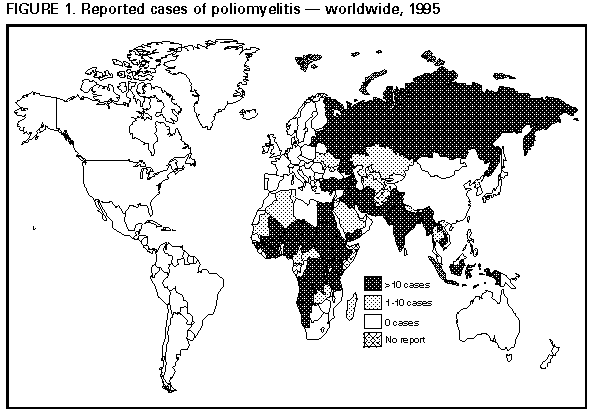
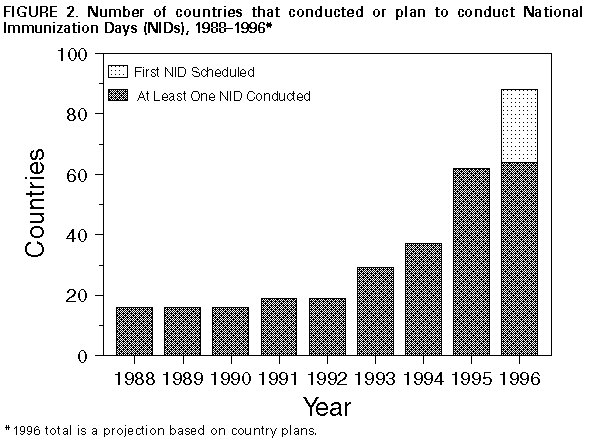
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Eradication of Poliomyelitis, 1995In 1988, the World Health Assembly established a target to eradicate poliomyelitis worldwide by the year 2000 (1). To achieve this goal, the World Health Organization (WHO) recommends four strategies: 1) achievement and maintenance of high routine vaccination coverage levels among children with at least three doses of oral poliovirus vaccine (OPV); 2) development of sensitive systems of epidemiologic and laboratory surveillance, including the use of the standard WHO case definition * ; 3) administration of supplementary doses of OPV to all young children (usually those aged <5 years) during National Immunization Days (NIDs) ** to rapidly interrupt poliovirus transmission; and 4) "mopping-up" vaccination campaigns localized campaigns targeted at high-risk areas where poliovirus transmission is most likely to persist at low levels. This report updates progress toward global polio eradication based on information submitted to WHO as of April 15, 1996. Worldwide. Routine vaccination coverage with three doses of OPV among children aged 1 year reached 83% in 1995, and ranged from 80% to 85% during 1990-1994. The provisional number of reported polio cases reached an all-time low of 6179 in 1995, representing a 28% decline from the 8635 cases reported in 1994, and an 82% decline from the 35,251 cases reported in 1988. In addition, the number of countries reporting zero cases of polio increased from 88 in 1988 to 150 in 1995 (Figure_1). The number of countries with endemic polio that conducted NIDs increased from 16 in 1988 to 62 in 1995. A total of 25 countries conducted their first NIDs during 1995, and 24 countries plan to conduct their first NIDs in 1996 (Figure_2). A total of 120 countries have implemented surveillance for acute flaccid paralysis (AFP) to detect all cases of polio that meet the standard WHO case definition and to monitor the circulation of wild polioviruses. Of these, 35 (29%) countries currently meet one performance indicator (i.e., an annual rate of one case of AFP per 100,000 population aged <15 years). WHO has certified six specialized reference laboratories, 12 regional reference laboratories, and 60 national laboratories as members of the Global Polio Laboratory Network. African Region. Polio remains endemic in most countries of West and Central Africa: in 1995, a total of 1512 cases of polio were reported, a decrease of 67% from 1988 (4564 cases). The number of countries reporting zero cases increased from eight in 1988 to 17 in 1995. Routine vaccination coverage increased to 58% in the region. During 1995, Algeria, Mauritania, and Namibia conducted NIDs, and Angola and South Africa conducted Sub-National Immunization Days (SNIDs). A total of 29 countries in the region plan to conduct either NIDs or SNIDs during 1996, and all polio-endemic countries intend to conduct NIDs during 1997. Region of the Americas. The last case of indigenous polio in the Americas was reported in 1991 from Peru, and in 1994, an international commission certified that indigenous transmission of wild poliovirus had been interrupted in the Americas (2). Eastern Mediterranean Region. From 1988 to 1995, the number of reported cases of polio decreased 68% (from 2339 to 738). In 1995, nine countries reported cases and 11 countries reported zero cases; three countries did not provide reports. Most (86%) cases in 1995 were reported by Pakistan (460 cases), Ir an (101), and Egypt (71). With the exception of Cyprus, Somalia, Sudan, and Yemen, all countries conducted NIDs in 1995 (3). In early 1996, a truce was declared in Sudan to facilitate NIDs; Yemen has scheduled NIDs for late 1996. European Region. From 1988 through 1995, the number of annually reported polio cases has remained stable: during 1995, a total of 205 cases were reported, compared with 214 cases in 1988. During 1995, the Russian Federation reported an outbreak of 154 cases, primarily from a region (Chechnya) affected by civil war; these cases accounted for 75% of the cases in the region. In 1995, a total of 10 countries conducted NIDs (Armenia, Azerbaijan, Bulgaria, Georgia, Kazakhstan, Kyrgyzstan, Tadjikistan, Turkmenistan, Turkey, and Uzbekistan) (3). NIDs were conducted in the Russian Federation during March and April 1996 and are planned for 1996 in Bosnia and Herzegovina, Moldova, and Ukraine; Romania and Yugoslavia (Serbia and Montenegro) plan to conduct SNIDs. Southeast Asian Region. From 1988 to 1995, the number of reported polio cases decreased 87%, from 25,711 to 3398. During 1995, India reported 3142 cases, representing 92% of the regional total and 51% of the global total. In 1995, six countries conducted NIDs (Bangladesh, Bhutan, India, Indonesia, Sri Lanka, and Thailand). India vaccinated 87.8 million children during NIDs in December 1995 (first round) and 93.6 million children in January 1996 (second round) (4). During 1996, the first NIDs have been conducted or are planned in the Democratic People's Republic of Korea, Myanmar, and Nepal. Western Pacific Region. From 1988 to 1995, the number of reported polio cases decreased 84%, from 2126 to 344. In 1995, polio was reported by five of the 35 countries in the region (Cambodia, People's Republic of China, Laos, Philippines, and Vietnam). The 91 cases in China represented a 98% decline from 1990 (5065 cases); all of the cases in 1995 were confirmed based on epidemiologic and clinical criteria, and no wild polioviruses were isolated despite substantial improvements in surveillance. However, one imported case of polio attributed to wild poliovirus was reported in the southwestern province of Yunnan, bordering Myanmar. Endemic polio confined to the Mekong Delta area was reported by Vietnam (133 cases) and Cambodia (105 cases). Philippines reported four cases that were confirmed on epidemiologic and clinical criteria; wild poliovirus was last isolated in Philippines in May 1993. Reported by: Pan American Health Organization, Washington, DC. Regional Office for Africa, Brazzaville, Congo; Regional Office for Eastern Mediterranean, Alexandria, Egypt; Regional Office for Europe, Copenhagen, Denmark; Regional Office for South East Asia, New Delhi, India; Regional Office for Western Pacific, Manila, Philippines; Global Program for Vaccines and Immunization, World Health Organization, Geneva, Switzerland. Respiratory and Enterovirus Br, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: Major achievements in the global campaign to eradicate polio include the substantial reduction in the global incidence of polio, the complete elimination of polio from the Region of the Americas, and the widespread implementation of NIDs and other WHO-recommended strategies. In particular, during 1995, all polio-endemic countries in Europe and Asia, with the exception of the Democratic People's Republic of Korea, Myanmar, Nepal, and Yemen, conducted NIDs, which provided supplemental poliovirus vaccine to nearly half of the world's children aged <5 years. During 1996, the Democratic People's Republic of Korea and Myanmar have conducted NIDs, and Nepal and Yemen plan to conduct NIDs. Substantial progress also has been reported in Africa, where routine vaccination coverage was>50% for the first time ever. More than half of the countries in Africa are planning to conduct NIDs or SNIDs in 1996. Barriers to global eradication of polio include financial, managerial, political, and technical challenges, and the need to implement the polio eradication strategies in the remaining polio-endemic countries, including those with internal conflicts and civil war. In 1995, countries of the Indian subcontinent accounted for approximately 60% of reported polio cases. In India, the next NIDs will be expanded to include children aged <5 years encompassing 125 million children. Bangladesh, India, Nepal, Pakistan, and Sri Lanka have scheduled synchronized NIDs in December 1996 and January 1997 to correspond with the cool and dry season, which should further improve the effectiveness of NIDs in interrupting poliovirus circulation, decreasing the incidence of polio in these countries and reducing the potential for exportation of polioviruses to polio-free areas of the world. Two geographically contiguous countries (Myanmar and Thailand) also will conduct NIDs during these months. In the African region, plans to conduct NIDs or SNIDs in 29 countries in 1996, and in all countries in the region by the end of 1997, pose exceptional challenges because of deficiencies in infrastructure for health, communications, and transportation. Substantial costs will be required to overcome these constraints. Most of the costs of polio eradication have been borne by individual countries; however, as the strategies for polio eradication are implemented in these poorest and least developed countries, a larger percentage of the costs will have to be procured through external sources. Rotary International, a major partner of the eradication initiative, is leading an international advocacy effort to expand the partnership of organizations and governments supporting the polio eradication initiative. The global eradication of polio by the year 2000 also will require that surveillance be strengthened to closely monitor the decline in polio incidence following NIDs and to target supplemental vaccination activities (i.e., "mopping-up"). An effective AFP surveillance system may require several years to implement and must be able to 1) detect one or more cases of AFP per 100,000 children aged <15 years; 2) collect stool specimens from>=80% of persons with AFP within 2 weeks of the onset of paralysis; 3) transport >=90% of stool specimens to the laboratory in satisfactory condition; and 4) isolate nonpolio enteroviruses from >=10% of stool specimens. References
* A confirmed case of polio is defined as acute flaccid paralysis (AFP) and at least one of the following: 1) laboratory-confirmed wild poliovirus infection, 2) residual paralysis at 60 days, 3) death, or 4) no follow-up investigation at 60 days. ** Mass campaigns over a short period (days to weeks) in which two doses of OPV are admin-istered to all children in the target age group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}