 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Factors Associated with Self-Perceived Excellent and Very Good Health Among Blacks -- Kansas, 1995Self-perceived health is related to functional status, morbidity, and mortality and is an important measure in determining health status and health-related quality of life (HRQOL) scales (1). In 1994, the group of health professionals who established the health status indicators for Healthy People 2000 (2) recommended that states examine the indicators for major demographic subgroups (e.g., racial/ethnic groups). The Kansas Department of Health and Environment (KDHE) analyzed data from the 1995 Behavioral Risk Factor Surveillance System (BRFSS) supplemental survey of blacks in Kansas to determine the relation between self-perceived excellent and very good health (EVGH) and physical functioning, mental functioning, role limitations, access to care, and health behaviors among blacks -- the largest racial/ethnic minority group in that state. This report summarizes the findings of the analysis, which indicate that several factors related to demographics, physical functioning, and health behaviors were associated with EVGH. BRFSS is a population-based, random-digit-dialed telephone survey of the non-institutionalized U.S. adult population aged greater than or equal to 18 years. In 1995, BRFSS was conducted in 50 states and provides population-based estimates of the prevalence of health behaviors, health-care access, and selected chronic conditions. Since 1993, BRFSS has included the option of a health status module (3-5). In Kansas, a supplemental survey to the statewide BRFSS was conducted in 1995 using all telephone prefixes having an estimated greater than or equal to 10% of households self-identified as black race based on 1990 census data. Self-identified blacks aged greater than or equal to 18 years (n=518; response rate=83%) participated in a structured interview that included the question, "Would you say in general your health is . . . excellent, very good, good, fair, or poor?" In addition, respondents were asked several questions about their health status, access to care, health behaviors, and demographics. All analyses were unweighted. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to measure the association between categorical variables and EVGH. A chi-square test for trend was conducted to determine whether income was associated with EVGH. Factors bivariately associated with EVGH were analyzed by sex-specific logistic regression models. Overall, the crude percentage of EVGH reported by blacks surveyed was 49% (54% of men and 47% of women); in comparison, 60% of whites surveyed in the 1995 statewide BRFSS reported EVGH (Figure_1). Annual household income less than $25,000 (OR=0.3, 95% CI=0.2-0.4) and reporting hypertension were negatively associated with EVGH among both black men and black women (OR=0.3, 95% CI=0.2- 0.4). The sex-specific percentage of EVGH varied by other demographic and descriptive characteristics (Table_1). Among women, factors positively associated with EVGH by bivariate analysis were working for wages (OR=2.0, 95% CI=1.2-3.3), being aged less than 45 years (OR=1.9, 95% CI=1.1-3.2), and reporting no days of poor physical health during the previous 30 days (OR=3.6, 95% CI=2.0- 6.4). Of the 10 factors negatively associated with EVGH among women by bivariate analysis, the association was strongest for having diabetes (OR=0.08, 95% CI=0.01-0.3), having any limitations (OR=0.2, 95% CI=0.05-0.4), and being unable to work (OR=0.2, 95% CI=0.02-0.7) (Table_1). Among men, factors positively associated with EVGH by bivariate analysis included working for wages (OR=2.2, 95% CI=1.2-4.2) and age less than 45 years (OR=2.7, 95% CI=1.5- 5.2). Of the eight factors negatively associated with EVGH among men by bivariate analysis, the association was strongest for being unable to work (OR=0.1, 95% CI=0.0-0.8), having any limitations (OR=0.2, 95% CI=0.05-0.4), and needing daily medications (OR=0.2, 95% CI=0.1-0.5) (Table_1). Because of interaction between sex, insurance status, and income with EVGH, sex-specific logistic regression models were constructed to adjust for factors independently associated with EVGH. Multivariate analysis indicated that, among women, factors negatively associated with EVGH included diabetes (OR=0.2, 95% CI=0.04-0.9), any limitations (OR=0.3, 95% CI=0.01-0.6), annual household income less than $25,000 (OR=0.3, 95% CI=0.2-0.5), hypertension (OR=0.4, 95% CI=0.2-0.8), and having smoked at least 100 cigarettes (OR=0.3, 95% CI=0.2-0.5). Among men, those with health insurance and an annual household income greater than or equal to $25,000 were 17 times more likely to report EVGH than those with no health insurance and an annual household income less than $25,000. Multivariate analysis indicated that factors negatively associated with EVGH among men included the duration of activity limitations in years (OR=0.8, 95% CI=0.7-1.0) and hypertension (OR=0.4, 95% CI=0.2-0.9). Reported by: M Perry, J Tasheff, P Marmet, C Miller, PhD, S Potsic, MD, G Pezzino, MD, State Epidemiologist, Kansas Dept of Health and Environment. Div of Health Promotion Statistics, Office of Analysis, Epidemiology, and Health Promotion, National Center for Health Statistics; State Br, Div of Applied Public Health Training (proposed), Epidemiology Program Office, CDC. Editorial NoteEditorial Note: Many of the national health objectives for the year 2000 are directed toward improving the health of U.S. minority populations. BRFSS is an effective means for states to measure and compare health outcomes and HRQOL among different groups. Kansas is the first state to report findings from a study using this approach to characterize factors associated with positive self-perceived health levels among racial/ethnic minority groups. In addition to this assessment of blacks, KDHE has implemented a similar supplemental BRFSS survey of Hispanics (the second largest and most rapidly increasing racial/ethnic minority group in the state). The finding that self-perceived EVGH was lower among blacks than among whites is consistent with mortality patterns in Kansas, which, when compared with those of whites, indicate the average age at death for black men and black women is 12.5 years younger and 13.4 years younger, respectively. The positive association between EVGH and an annual household income greater than or equal to $25,000 for both black men and black women underscores previous studies indicating the impact of economics on self-perceived health status (6). In addition, the findings suggest that efforts to improve the health status of blacks and, therefore, self-perceived health and HRQOL, should be directed toward preventing activity limitations and hypertension among men and toward preventing diabetes, smoking initiation, and activity limitations among women. The findings in this report are subject to at least five limitations. First, temporal variations in the relation between variables associated with EVGH have not been characterized, and the potential for increasing self-perceived EVGH by altering these factors is unknown. Second, many of the biologically and psychologically plausible determinants of EVGH (e.g., chronic conditions such as heart disease, cancer, and arthritis) were not associated with EVGH, probably reflecting the small sample size or misclassification. Third, the findings of the study may not be generalizable to all blacks in the state because black households without telephones and those in areas of the state with less than 10% of the households self-identified as black were not eligible for survey selection. Fourth, identification of self-perceived health status may vary by cultural groups, and comparisons of that status across groups may reflect cultural differences rather than health status. Finally, the factors studied were chosen based on hypotheses, some limited literature, and available data and were not identified by the respondents as factors important to them and their health status. The relation between the duration of activity limitations and EVGH among black men in Kansas suggests the need to better characterize the types and causes of activity limitations among this group to enable development of appropriate interventions. The findings also suggest that, for some women, strategies for improving self-perceived health might include programs for diabetes self-management, education of health-care providers, prevention of smoking initiation, and promotion of general health. KDHE, in collaboration with an advisory group to the BRFSS supplemental survey of blacks, is implementing interventions to improve HRQOL among black residents of Kansas. Examples of such efforts include extended diabetes outreach and education to black women and the involvement of churches to reach both men and women with hypertension. KDHE is planning future BRFSS surveys to assess the impact of these programs. References
Figure_1 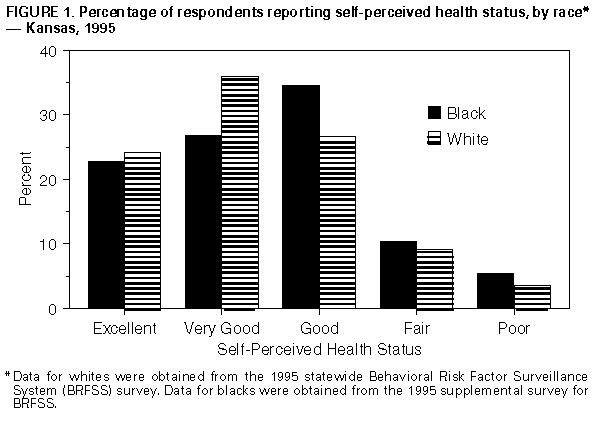 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Unweighted percentage of black survey respondents who reported excellent
or very good health (EVGH), by sex and selected characteristics -- supplemental
Behavioral Risk Factor Surveillance System survey, Kansas, 1995 *
====================================================================================================
Men (n=207) Women (n=311)
------------------------------ -------------------------------
Sample Sample
Characteristic size (%) (95% CI +) size (%) (95% CI)
--------------------------------------------------------------------------------------------------
Age group (yrs) &
18-24 37 (64.9) (47.5%-79.8%) 59 (55.9) (42.4%-68.8%)
25-44 92 (62.0) (51.2%-71.9%) 154 (50.0) (41.8%-58.2%)
45-64 60 (43.3) (30.6%-56.8%) 63 (41.3) (29.0%-54.4%)
65-74 11 (18.2) ( 2.3%-51.8%) 23 (21.7) ( 7.5%-43.7%)
>= 75 5 (20.0) ( 0.5%-71.6%) 10 (40.0) (12.2%-73.8%)
Education level &
Less than high school 27 (25.9) (11.1%-46.3%) 30 (36.7) (19.9%-56.1%)
High school graduate 68 (50.0) (37.6%-62.4%) 123 (37.4) (28.8%-46.6%)
Some college 70 (62.9) (50.5%-74.1%) 103 (54.4) (44.3%-64.2%)
College graduate 40 (62.5) (45.8%-77.3%) 53 (60.4) (46.0%-73.5%)
Annual household income @
<$14,999 15 (33.3) (11.8%-61.6%) 35 (22.9) (10.4%-40.1%)
$15,000-$24,999 63 (34.9) (23.3%-48.0%) 119 (37.0) (28.3%-46.3%)
$25,000-$49,999 83 (68.7) (57.6%-78.4%) 93 (66.7) (56.1%-76.1%)
>= $50,000 28 (67.9) (47.6%-84.1%) 34 (52.9) (35.1%-70.2%)
Employment status &
Employed 154 (60.4) (52.2%-68.2%) 199 (54.3) (47.1%-61.3%)
Unemployed 12 (41.7) (15.2%-72.3%) 22 (36.4) (17.2%-59.3%)
Homemaker 0 -- -- 16 (43.8) (19.8%-70.1%)
Student 7 (71.4) (29.0%-96.3%) 20 (50.0) (27.2%-72.8%)
Retired 23 (26.1) (10.2%-48.4%) 36 (27.8) (14.2%-45.2%)
Unable to work 9 (11.1) ( 0.3%-48.2%) 16 (12.5) ( 1.6%-38.3%)
Marital status &
Married 78 (52.6) (40.9%-64.0%) 99 (53.5) (43.2%-63.6%)
Divorced 38 (57.9) (40.8%-73.7%) 70 (43.6) (32.4%-56.7%)
Widowed 9 (44.4) (13.7%-78.8%) 31 (29.0) (14.2%-48.0%)
Separated 10 (30.0) ( 6.7%-65.2%) 18 (38.9) (17.3%-64.3%)
Never married 60 (58.3) (44.9%-70.9%) 85 (45.9) (35.0%-57.0%)
Unmarried couple 10 (50.0) (18.7%-81.3%) 6 (50.0) (11.8%-88.2%)
Have health insurance &
Yes 175 (53.7) (46.0%-61.3%) 260 (45.8) (39.6%-52.0%)
No 30 (53.3) (34.3%-71.7%) 49 (53.1) (38.3%-67.5%)
Needed to see a doctor
but didn't because
of cost
Yes 25 (48.0) (27.8%-68.7%) 49 (28.6) (16.6%-43.3%)
No 180 (54.4) (46.9%-61.9%) 260 (50.4) (44.1%-56.6%)
Have diabetes &
Yes 7 (14.3) ( 0.4%-57.9%) 24 ( 4.2) ( 0.1%-21.1%)
No 198 (55.1) (47.8%-62.1%) 285 (50.5) (44.6%-56.5%)
Have hypertension &
Yes 63 (31.7) (20.6%-44.7%) 112 (28.6) (20.4%-37.9%)
No 142 (63.4) (54.9%-71.3%) 197 (57.4) (50.1%-64.4%)
Have high blood
cholesterol level &
Yes 35 (42.9) (26.3%-60.6%) 51 (31.4) (19.1%-45.9%)
No 170 (55.9) (48.1%-63.5%) 258 (50.0) (43.7%-56.3%)
Take daily medications
Yes 47 (27.7) (15.6%-42.6%) 84 (25.0) (16.2%-35.6%)
No 158 (61.4) (53.3%-69.0%) 225 (55.1) (48.4%-61.7%)
Have any activity
limitation &
Yes 47 (31.9) (19.1%-47.1%) 78 (25.6) (16.4%-36.8%)
Duration <= 1 yr 22 (45.4) (22.4%-67.8%) 34 (38.2) (22.2%-56.4%)
2-4 yrs 10 (40.0) (12.2%-73.8%) 20 (15.0) ( 3.2%-37.9%)
>= 5 yrs 15 ( 6.7) ( 0.2%-31.9%) 24 (16.7) ( 4.7%-37.4%)
No 158 (60.1) (52.0%-67.8%) 231 (54.1) (47.5%-60.7%)
Have smoked >= 100
cigarettes during
lifetime **
Yes 111 (50.5) (40.8%-60.1%) 188 (36.1) (29.3%-43.5%)
No 93 (58.1) (47.4%-68.2%) 122 (54.3) (44.8%-63.2%)
--------------------------------------------------------------------------------------------------
* n=518.
+ Confidence interval.
& Excludes two men and two women for whom this characteristic was missing.
@ Excludes 18 men and 30 women for whom either EVGH or income data were missing.
** Excludes three men and one woman for whom either EVGH or smoking data were missing.
====================================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}