 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Injuries and Deaths Associated with Use of Snowmobiles -- Maine, 1991-1996During the 1995-96 winter season (i.e., November 1995 through April 1996), both the Maine Department of Inland Fisheries and Wildlife (DIFW) and the Maine Office of the Chief Medical Examiner (OCME) detected an increase in deaths associated with snowmobile use in Maine. From the fall of 1991 through the spring of 1995, three to eight snowmobile-related deaths occurred each winter season (mean: 5.4 per winter season); during the 1995-96 winter season, 12 deaths were recorded -- the largest number of snowmobile-related deaths in 25 years. In addition, from 1991 through 1996, the number of registered snowmobiles increased from 61,641 to a record high of 76,477, respectively, and the death rate per registered vehicle in 1996 was higher than in any of the previous 5 years (Figure_1). To assist in the development and evaluation of strategies to prevent injury and death associated with the use of snowmobiles in Maine, the Bureau of Health, Maine Department of Human Services (BOH), collaborated with DIFW and OCME to examine data about fatal and nonfatal injuries associated with use of snowmobiles from 1991 through 1996. This report summarizes the results of this analysis and recommends strategies for preventing such deaths and injuries. Maine state law requires snowmobile operators (residents and nonresidents) to report all incidents involving snowmobiles that result in injury requiring medical attention or in property damage of greater than or equal to $300. * DIFW wardens or other law-enforcement officers investigate all reported incidents and collect data about the time of occurrence, weather conditions, terrain, alcohol use, helmet use, and cause and circumstances. Data about snowmobile-associated fatalities were obtained from BOH death certificates (age, sex, residence, education, and marital status) and from a computerized database at the OCME (blood or vitreous alcohol levels and cause of death). Characteristics of Incidents For the winter seasons of 1990-91 through 1995-96, a total of 1355 snowmobile-related incidents were investigated (range: 173 {1992} to 285 {1996}, mean: 226 per season). These 1355 incidents involved 1828 snowmobiles and resulted in 903 injuries among 2105 operators and passengers. A total of 1565 (86%) of the snowmobile operators were male. Of the 1740 operators for whom age was known, 1076 (62%) were aged greater than 25 years. Of the 1817 operators and passengers for whom information was available, 1312 (72%) were wearing helmets at the time of the incident. Weather conditions were known for 1263 incidents, of which 1002 (79%) occurred during clear weather; terrain was known for 1253 incidents, of which 535 (43%) occurred on marked and groomed snowmobile trails. Of the 1307 incidents for which time of incident was known, 652 (50%) occurred during darker hours (i.e., 4 p.m.-6 a.m.). The primary causes of the incidents were known for 1311 incidents and included excessive speed (684 {52%}), inattention or careless operation (350 {27%}), mechanical failure (82 {6%}), operating on a public way (32 {2%}), operating on a steep hill or snow bank (28 {2%}), crossing unsafe ice (18 {1%}), and other (117 {9%}). Of 1307 incidents for which data on type of incident were available, 301 (23%) were falls off the snowmobile, 283 (22%) were collisions with another snowmobile, 201 (15%) were collisions with trees, 187 (14%) were collisions with a rock or other object, 97 (7%) were falls off a bank or sudden drop in terrain, 40 (3%) were collisions with another motor vehicle, and 25 (2%) were falls through ice. The role of alcohol had been evaluated for 1255 incidents, and alcohol was determined to be a contributing factor in 159 (13%) of these incidents. Of the 903 injuries, 282 (31%) involved a lower extremity, 165 (18%) an upper extremity, 151 (17%) the head or neck, 79 (9%) the chest or trunk, and 63 (7%) the back; for the remaining 163 (18%), the location of injury was not specified. Specific types of injuries included fractures (32%); lacerations (10%); contusions (7%); concussions (4%); abrasions (3%); dislocations (2%); burns (2%); exposure (1%); sprains (1%); internal or puncture (less than 1%); drowning (less than 1%); and unspecified, other, or unknown (37%). Deaths During 1991-1996, a total of 39 deaths were associated with snowmobile use, of which 32 (82%) resulted from trauma and seven from drowning; 37 (95%) decedents were male, and 16 (41%) were married. Thirty (77%) of the 39 decedents were residents of Maine. At the time of the incident, 37 decedents were operating the snowmobile, and two were passengers. The median age of decedents was 34 years (range: 12-69 years). Decedents who had been operating the snowmobile were more likely to be aged greater than 25 years (86%) than operators involved in all (fatal or nonfatal) incidents (62%). For the 37 decedents for whom data were available, the median number of years of education was 12 (range: 5-16 years). Of the 31 decedents for whom data were available, 25 (81%) were wearing helmets at the time of the incident. Alcohol levels were obtained for 37 decedents; of these, either blood or vitreous alcohol levels were greater than 0.08 g/dL in 15 (41%). Fatal incidents were more likely to occur during darker hours of the day (4 p.m.-6 a.m.). Reported by: D Tourtelotte, J Ross, Maine Dept of Inland Fisheries and Wildlife; H Ryan, Maine Office of the Chief Medical Examiner; E Naor, N Bartlett, Office of Health Data and Program Management, Bur of Health, Maine Dept of Human Svcs. Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control; Div of Health Promotion Statistics, National Center for Health Statistics, CDC. Editorial NoteEditorial Note: The findings in this report indicate that most snowmobile-associated incidents in Maine during 1991-1996 resulted from collisions caused by excessive speed and careless operation of the vehicle. The high proportion of incidents that occurred during darker periods underscores the importance of increased caution during such periods and the need to evaluate the effect of snowmobile characteristics (e.g., headlight luminance) in reducing the hazards of operating snowmobiles at nighttime. In addition, alcohol was determined to be a factor in 13% of all incidents, and elevated alcohol levels were detected in 41% of all decedents; although blood alcohol levels were not measured in the operators involved in all snowmobile-associated incidents, these findings suggest an increased risk for fatal injury associated with alcohol use while operating a snowmobile. In a previous report from New Hampshire, the prevalence of alcohol use was substantially lower among self-reported snowmobile incidents than among police-reported incidents (1). However, in Maine, determinations about the role of alcohol were made by law-enforcement officers for all reported incidents. The findings in this report are subject to at least two limitations. First, because levels of snowmobile use vary in relation to snowfall and other weather conditions and because not all nonresidents are required to register their snowmobiles in Maine, snowmobile registrations are only a crude approximation of actual use of snow-mobiles; rates of incidents or deaths based on snowmobile-miles driven or hours of use could not be determined. Second, because DIFW surveillance statistics had been summarized annually, the OCME data and death-certificate data were compared with all snowmobile-associated incidents reported to DIFW rather than to nonfatal incidents only. In addition, factors associated with property damage could not be differentiated from those associated with injury. Because risk factors associated with property damage may differ from those associated with injury incidents, the findings may not accurately reflect risks for injuries. For example, if alcohol contributed disproportionately to injury-producing incidents, the aggregate analysis would have resulted in an underestimation of the contribution of alcohol to injuries. The results of this investigation suggest that educational interventions to reduce snowmobile-associated injury and death should focus on promoting more cautious snowmobile operation and reducing the use of alcohol while operating a snowmobile. A previous report from New Hampshire indicated that most snowmobile-related deaths occurred among males in their 20s and suggested targeting interventions (e.g., operator safety courses) at males aged less than 30 years (1); however, the findings in this report suggest that the target population should be broadened to include older men with families. The effectiveness of educational efforts should be compared with other interventions such as limiting vehicle horsepower and velocity potential or increased regulation and enforcement of operating speed limits. The findings in this report will be incorporated into a statewide strategic plan in Maine to improve snowmobile safety. Efforts will include safety education programs in collaboration with local snowmobiling associations, placing warning signs at strategic locations on snowmobile trails, and establishing local snowmobile safety-check stations. Reference
* MRSA Title 12, *** 7827, **** 22A and B. Figure_1 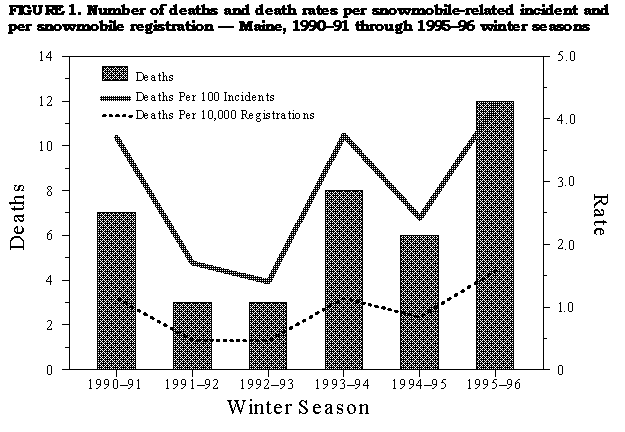 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}