 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Rates of Homicide, Suicide, and Firearm-Related Death Among Children -- 26 Industrialized CountriesDuring 1950-1993, the overall annual death rate for U.S. children aged less than 15 years declined substantially (1), primarily reflecting decreases in deaths associated with unintentional injuries, pneumonia, influenza, cancer, and congenital anomalies. However, during the same period, childhood homicide rates tripled, and suicide rates quadrupled (2). In 1994, among children aged 1-4 years, homicide was the fourth leading cause of death; among children aged 5-14 years, homicide was the third leading cause of death, and suicide was the sixth (3). To compare patterns and the impact of violent deaths among children in the United States and other industrialized countries, CDC analyzed data on childhood homicide, suicide, and firearm-related death in the United States and 25 other industrialized countries for the most recent year for which data were available in each country (4). This report presents the findings of this analysis, which indicate that the United States has the highest rates of childhood homicide, suicide, and firearm-related death among industrialized countries. In the 1994 World Development Report (5), 208 nations were classified by gross national product; from that list, the United States and all 26 of the other countries in the high-income group and with populations of greater than or equal to 1 million were selected because of their economic comparability and the likelihood that those countries maintained vital records most accurately. In January and February 1996, the ministry of health or the national statistics institute in each of the 26 countries were asked to provide denominator data and counts by sex and by 5-year age groups for the most recent year data were available for the number of suicides (International Classification of Diseases, Ninth Revision {ICD-9}, codes E950.0-E959), homicides (E960.0-E969), suicides by firearm (E955.0-E955.4), homicides by firearm (E965.0-E965.4), unintentional deaths caused by firearm (E922.0-E922.9), and firearm-related deaths for which intention was undetermined (E985.0-E985.4); 26 (96%) countries, including the United States, provided complete data *. Twenty (77%) countries provided data for 1993 or 1994; the remaining countries provided data for 1990, 1991, 1992, or 1995. Cause-specific rates per 100,000 population were calculated for three groups (children aged 0-4 years, 5-14 years, and 0-14 years). The rates for homicide and suicide by means other than firearms were calculated by subtracting the firearm-related homicide and firearm-related suicide rates from the overall homicide and suicide rates. Rates for the United States were compared with rates based on pooled data for the other 25 countries. Of the 161 million children aged less than 15 years during the 1 year for which data were provided, 57 million (35%) were in the United States and 104 million (65%) were in the other 25 countries. Overall, the data provided by the 26 countries included a total of 2872 deaths among children aged less than 15 years for a period of 1 year. Homicides accounted for 1995 deaths, including 1177 (59%) in boys and 818 (41%) in girls. Of the homicides, 1464 (73%) occurred among U.S. children. The homicide rate for children in the United States was five times higher than that for children in the other 25 countries combined (2.57 per 100,000 compared with 0.51) (Table_1). Suicide accounted for the deaths of 599 children, including 431 (72%) in boys and 168 (28%) in girls. Of the suicides, 321 (54%) occurred among U.S. children. The suicide rate for children in the United States was two times higher than that in the other 25 countries combined (0.55 compared with 0.27) (Table_1). No suicides were reported among children aged less than 5 years. A firearm was reported to have been involved in the deaths of 1107 children; 957 (86%) of those occurred in the United States. Of all firearm-related deaths, 55% were reported as homicides; 20%, as suicides; 22%, as unintentional; and 3%, as intention undetermined. The overall firearm-related death rate among U.S. children aged less than 15 years was nearly 12 times higher than among children in the other 25 countries combined (1.66 compared with 0.14) (Table_1). The firearm-related homicide rate in the United States was nearly 16 times higher than that in all of the other countries combined (0.94 compared with 0.06); the firearm-related suicide rate was nearly 11 times higher (0.32 compared with 0.03); and the unintentional firearm-related death rate was nine times higher (0.36 compared with 0.04). For all countries, males accounted for most of the firearm-related homicides (67%), firearm-related suicides (77%), and unintentional firearm-related deaths (89%). The nonfirearm-related homicide rate in the United States was nearly four times the rate in all of the other countries (1.63 compared with 0.45), and nonfirearm-related suicide rates were similar in the United States and in all of the other countries combined (0.23 compared with 0.24). The rate for firearm-related deaths among children in the United States (1.66) was 2.7-fold greater than that in the country with the next highest rate (Finland, 0.62) (Figure_1). Except for rates for firearm-related suicide in Northern Ireland and firearm-related fatalities of unknown intent in Austria, Belgium, and Israel, rates for all types of firearm-related deaths were higher in the United States than in the other countries. However, among all other countries, the impact of firearm-related deaths varied substantially. For example, five countries, including three of the four countries in Asia, reported no firearm-related deaths among children. In comparison, firearms were the primary cause of homicide in Finland, Israel, Australia, Italy, Germany, and England and Wales. Five countries (Denmark, Ireland, New Zealand, Scotland, and Taiwan) reported only unintentional firearm-related deaths. Reported by: Div of Violence Prevention, National Center for Injury Prevention and Control, CDC. Editorial NoteEditorial Note: The findings in this report document a high rate of death among U.S. children associated with violence and unintentional firearm-related injuries, particularly in comparison with other industrialized countries. Even though rates in all other countries were lower than those in the United States, rates among other countries varied substantially and were particularly low in some countries. Although specific reasons for the differences in rates among countries are unknown, previous studies have reported on the associations between rates of violent childhood death and low funding for social programs (6), economic stress related to participation of women in the labor force (7,8), divorce, ethnic-linguistic heterogeneity, and social acceptability of violence (9). The findings of the analysis in this report are subject to at least three limitations. First, although the data were obtained from official sources and were based on ICD-9 codes, the sensitivity and specificity of the vital records and reporting systems may have varied by country. Second, because 21 (81%) countries each reported less than 10 firearm-related deaths among children aged 0-14 years, the firearm-related death rates for those countries, when not pooled, are unstable and may vary substantially for different years. Finally, only one half of the countries (including the United States) reported all four digits of the ICD-9 codes for firearm-related deaths; the fourth digit distinguishes whether deaths were caused by injuries from firearms or by other explosives. For countries in which this distinction could not be made, the firearm-related death rates may be overestimated slightly. In May 1996, the 49th World Health Assembly adopted a resolution that declared violence a leading worldwide public health problem and urged all member states to assess the problem of violence and to communicate their findings to the World Health Organization (10). Cross-cultural comparisons may identify key factors (e.g., attitudinal, behavioral, educational, socioeconomic, or regulatory) not evident from intranational studies that could assist in the development of new country-specific strategies for preventing such deaths. References
* Complete data were provided by Australia, Austria, Belgium, Canada, Denmark, England and Wales, Finland, France, Germany, Hong Kong, Ireland, Israel, Italy, Japan, Kuwait, Netherlands, New Zealand, Northern Ireland, Norway, Scotland, Singapore, Sweden, Spain, Switzerland, Taiwan, and the United States. In this analysis, Hong Kong, Northern Ireland, and Taiwan are considered as countries. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Rates * of homicide, suicide, and firearm-related death + among children aged <15 years -- United States and 25 other industrialized countries &
=================================================================================================================================================================
Firearm-related deaths
------------------------------------------------------------------------------------------------------
Age group (yrs) Total homicide Total suicide Homicide Suicide Unintentional Intention undetermined Total
-----------------------------------------------------------------------------------------------------------------------------------------------------------------
0-4
U.S. 4.10 0 0.43 0 0.15 0.01 0.59
Non-U.S. 0.95 0 0.05 0 0.01 0.01 0.07
Ratio U.S.:Non-U.S. 4.3:1 8.6:1 15.0:1 1.0:1 8.4:1
5-14
U.S. 1.75 0.84 1.22 0.49 0.46 0.06 2.23
Non-U.S. 0.30 0.40 0.07 0.05 0.05 0.01 0.18
Ratio U.S.:Non-U.S. 5.8:1 2.1:1 17.4:1 9.8:1 9.2:1 6.0:1 12.4:1
0-14
U.S. 2.57 0.55 0.94 0.32 0.36 0.04 1.66
Non-U.S. 0.51 0.27 0.06 0.03 0.04 0.01 0.14
Ratio U.S.:Non-U.S. 5.0:1 2.0:1 15.7:1 10.7:1 9.0:1 4.0:1 11.9:1
-----------------------------------------------------------------------------------------------------------------------------------------------------------------
* Per 100,000 children in each age group and for 1 year during 1990-1995.
+ Homicides (International Classification of Diseases, Ninth Revision, codes E960.0-E969), sui-cides (E950.0-E959), homicides by firearm (E965.0-E965.4),
suicides by firearm (E955.0- E955.4), unintentional deaths caused by firearm (E922.0-E922.9), and firearm-related deaths for which intention was undetermined
(E985.0-E985.4).
& All countries classified in the high-income group with populations 31 million ( 5 ) that provided complete data (Australia, Austria, Belgium, Canada, Denmark,
England and Wales, Finland, France, Germany, Hong Kong, Ireland, Israel, Italy, Japan, Kuwait, Netherlands, New Zealand, Northern Ireland, Norway, Scotland,
Singapore, Sweden, Spain, Switzerland, and Taiwan). In this analysis, Hong Kong, Northern Ireland, and Taiwan are considered as countries.
=================================================================================================================================================================
Return to top. Figure_1 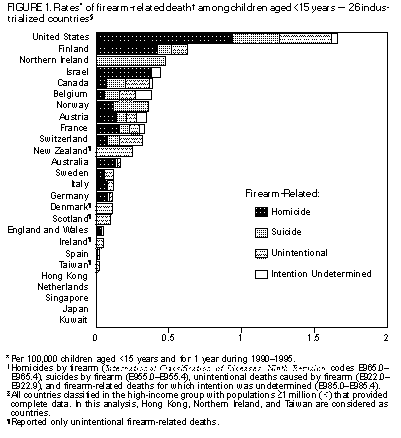 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}