 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
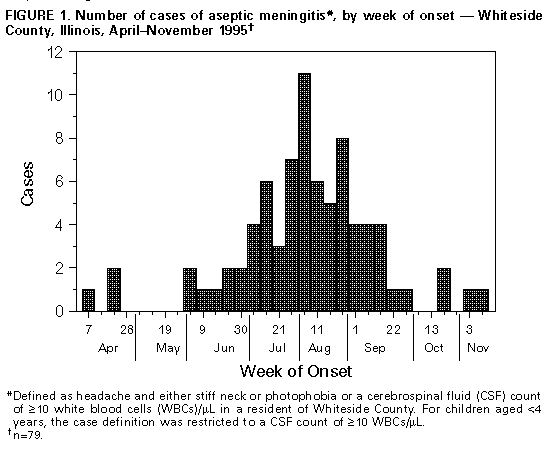
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Aseptic Meningitis -- Whiteside County, Illinois, 1995Aseptic meningitis (AM) is a severe, nonbacterial infection of the central nervous system that affects an estimated 30,000-50,000 persons each year in the United States (1). On July 21, 1995, the infection-control coordinator of the county hospital in Whiteside County (1990 population: 60,000), Illinois, reported to CDC an outbreak of AM. From June 7 through July 21, 1995, a total of 29 persons had onset of clinical AM, characterized by fever, headache, stiff neck, and photophobia. Many cases had cerebrospinal fluid (CSF) pleocytosis, and all had negative bacterial cultures. Preliminary identification of an enterovirus was made from virus-isolation studies. This report describes the investigation of this outbreak by county and state health officials, which indicated that, although members of the community were concerned about possible transmission at large public gatherings and several swimming locations, there was no risk for illness in these settings. Whiteside County is located in northwestern Illinois and has an industrial and agricultural economic base. Nearly two thirds (65%) of the population is concentrated in the eastern third of the county, where the two largest towns (Sterling and Rock Falls) are located. Information about all suspected cases of AM and all lumbar-puncture procedures documented during April-November 1995 was obtained through hospital chart review and by contacting physicians in private practice. A case of AM was defined as headache and either stiff neck or photophobia or a CSF count of greater than or equal to 10 white blood cells (WBCs)/uL in a resident of Whiteside County. For children aged less than 4 years, the case definition was restricted to a CSF count of greater than or equal to 10 WBCs/uL. For persons who had onset of illness during June 1-August 4, 1995 (the peak period of recreational water use), a matched case-control study was conducted to determine whether illness was associated with attendance at large public events, swimming in public swimming locations, or potential household risk factors. Two controls per case were selected by asking case-patients or their guardians to identify casual acquaintances of the same sex and age. CSF and/or stool specimens were obtained from patients during their acute illness for enteroviral isolation studies. During April-November, 79 cases of AM were identified in Whiteside County (Figure_1). In contrast, during 1990-1994, the annual reported number of cases in the county ranged from zero to seven. The illness rate was substantially higher in Sterling and Rock Falls (22.4 per 10,000 population) than in the remainder of the county (3.7 per 10,000 population). Of 79 case-patients, 41 (52%) were male. The median age was 21 years (range: 0-66 years), with similar rates of illness in all age groups for patients aged less than or equal to 50 years; only two patients were aged greater than 50 years. Symptoms most commonly reported by case-patients included headache (100%), stiff neck (78%), fever (76%), nausea or vomiting (75%), muscle aches (57%), and photophobia (42%). Sixty-four patients were hospitalized, and 15 were treated as outpatients (eight in the emergency department and seven in physicians' offices). Lumbar punctures were performed on 66 (84%) of 79 case-patients. Of the 66 CSF specimens obtained from case-patients, 37 (56%) had WBC counts of greater than or equal to 10 WBCs/uL; all CSF cultures were negative for bacterial pathogens. Echovirus type 9 was the predominant agent identified from case-patients and was isolated from six (9%) of 66 CSF specimens and three (19%) of 16 stool specimens. In addition, echovirus types 5 and 21 were isolated from one stool specimen. The remaining 11 stool and 60 CSF specimens were either negative or of insufficient quantity for virus isolation. Of the 79 case-patients, 37 (47%) had onset of illness during June 1-August 4 and were included in the case-control study. The investigation included potential risk factors in the community and in households. Illness was not associated with attendance at any of eight public events (e.g., Independence Day fireworks in Rock Falls) (p=0.9). Similarly, no association was found between illness and participation in swimming, frequency of swimming, location of any swimming, or location of usual swimming (all p greater than 0.5). In addition, no association was found between illness and other possible risk factors (e.g., source of household drinking water; household presence of children in diapers or children in day care; or occupation in health-care services, day care, or food handling and preparation) (all p greater than 0.2). Reported by: A Rodriguez, MPH, Whiteside County Health Dept, Morrison; S Westbo, CGH Medical Center, Sterling; B Adam, C Langkop, MSPH, BJ Francis, MD, State Epidemiologist, Illinois Dept of Public Health. Program Svcs and Development Br, Div of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion; Respiratory and Enteroviruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: The etiologic agent identified in this outbreak was an enterovirus (echovirus type 9), the only virus isolated from CSF. Echovirus type 9 was the predominant enterovirus reported during the summer of 1995 by state health laboratories to CDC (CDC, unpublished data, 1995). Other echoviruses (e.g., serotypes 5 and 21) were identified from stool specimens; however, enteroviruses frequently cocirculate in a community (1,2). The rates of isolation of echovirus 9 from stool and CSF specimens of case-patients (19% and 9%, respectively) were lower than those obtained in previous investigations, possibly resulting from the timing of sample collection following onset of illness; the small volume of sample obtained; or loss of virus in the specimen during handling, storage, or shipment. Transmission of enteroviruses usually is person-to-person, either through the fecal-oral or oral-oral routes. Although enteroviruses can be readily isolated from waste waters and occasionally from recreational waters, studies examining the association of enteroviral illness with recreational water use have obtained varying results. An unusual point-source contamination of a swimming facility in England resulted in an outbreak of echovirus 30 illness: on opening day of the facility, a swimmer became ill and vomited into the pool, which had been inadequately chlorinated; subsequently, other swimmers became ill (3). In a study in Wisconsin, an association was found between summertime recreational water use and visits to a pediatric office for milder "enteroviral illness" (4). In a study of an outbreak of AM at a boys' camp in New York state, coxsackie B5 was isolated from lake water; however, because most of the ill campers shared the same cabin and had multiple opportunities for person-to-person spread, the investigation determined this was the most likely route of transmission (5). Similarly, in the investigation reported here, no association was found between illness and recreational water use, other community risk factors (e.g., attendance at public events), or household risk factors. Failure of the investigation to find an association with either community or household factors may have resulted from a focus on enteroviral illness rather than infection, the small numbers of persons studied, or the high frequency with which persons participated in the community activities investigated. The outbreak may have been caused by person-to-person transmission rather than communal contamination. Enteroviral illness and AM typically demonstrate a seasonal pattern, with the highest incidence occurring during the summer and fall months (1). This community outbreak occurred during the usual season of greatest enterovirus activity. The magnitude of the outbreak may have been greater than usual because of circulation of a serotype or strain of enterovirus not common to northwestern Illinois and for which little immunity existed in the population. AM outbreaks caused by entoviruses, such as the one in Whiteside County, underscore the importance of public health messages that emphasize the role of personal hygiene (e.g., regular handwashing and avoiding sharing of eating utensils and drinking containers) in interrupting transmission of enterovirus infections. Health departments should target messages about hygiene to high-risk populations (e.g., day care centers, families with children in diapers, schools with young children, and school athletic teams). References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}