 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication -- Africa, 1996In 1988, the World Health Assembly established a goal of eradicating poliomyelitis worldwide by the year 2000 (1). The four strategies recommended by the World Health Organization (WHO) for polio eradication are 1) achieving and maintaining high routine vaccination coverage levels among children aged less than 1 year with at least three doses of oral poliovirus vaccine (OPV); 2) developing sensitive systems of epidemiologic and laboratory surveillance, including establishing acute flaccid paralysis (AFP) surveillance *; 3) administering supplementary doses of OPV to all young children (usually those aged less than 5 years) during National Immunization Days ** (NIDs) to rapidly interrupt wild poliovirus transmission; and 4) conducting "mopping-up" vaccination campaigns -- localized campaigns targeting high-risk areas where poliovirus transmission is most likely to persist at low levels. Eradicating polio from Africa remains one of the major challenges to global eradication by the target date. This report summarizes progress achieved in 1996 toward polio eradication in Africa with the implementation of supplemental vaccination activities; the reported OPV coverage during the NIDs or Subnational Immunization Days (SNIDs) was greater than 80% in the target age group in most countries (Table_1), and the estimated cost was 50[ per child vaccinated during NIDs. In 1995, a total of 2192 polio cases were reported from the 46 countries in the African Region of WHO. During the same year, 16 countries, including four of the largest (Angola, Ethiopia, Nigeria, and Zaire), reported that less than 50% of children had received three doses of OPV through routine vaccination services. The first round of NIDs and SNIDs in the African Region (Figure_1) were conducted from January 1996 through March 1997. In the largest series of vaccination days conducted in Africa during a single year, approximately 74 million children -- approximately three fourths of all children aged less than 5 years in Africa -- were targeted to receive supplemental doses of OPV. By March 1997, a total of 31 countries had finished or were completing these supplemental vaccination activities; NIDs were being or had been conducted in 27 (87%) countries, and SNIDs were conducted in four (13%) -- Gabon (targeting 23% of all children aged less than 5 years), Zaire (21%), Mozambique (16%), and Ethiopia (3%). SNIDs in the larger countries with difficult circumstances (Ethiopia and Zaire) served a dual purpose of providing supplemental OPV doses to urban children at highest risk for polio and strengthening planning and logistics for the 1997 vaccination days. Reported OPV coverage after each round of NIDs or SNIDs was greater than or equal to 80% in the target age group in most countries (Table_1). OPV coverage of less than 80% during at least one round was reported from Angola, Eritrea, Gabon, Kenya, Lesotho, Malawi, Nigeria, Rwanda, and South Africa; coverage data were unavailable from Cameroon and Central African Republic. The first round of vaccination days reached approximately 80% of the target children in most countries, and reported coverage was higher in the second round in almost every country. For 20 countries with information about the total number of children who were vaccinated in both rounds, 18 (90%) of 20 countries reached more children in the second round; in 10 (50%) of 20 countries, the coverage in the second round was at least 5% higher than in the first round. In Nigeria, OPV coverage increased by 17 percentage points in the second round (64%) compared with the first round (47%). Of the 32 states in Nigeria, 11 were selected and provided technical assistance by WHO and the United Nations Children's Fund (UNICEF). In these 11 states, coverage in the first round was 63% and in the second round was 93%. During April-December 1997, supplemental vaccination activities for polio eradication will be conducted for the first time in Burundi, Gambia, Guinea, Guinea-Bissau, Liberia, Madagascar, Mali, Niger, Senegal, and Sierra Leone. This will bring the total number of countries participating to 41 of the 46 countries in the African Region. In addition, Ethiopia, Gabon, and Mozambique will conduct NIDs, and countries that conducted NIDs in 1996 plan to conduct NIDs in 1997. Zaire may extend SNIDs to target half the country. Surveillance for AFP and wild poliovirus began in approximately half of the countries in 1996. Wild poliovirus genomic sequencing was performed on at least one poliovirus isolate from each of 14 countries, including the four countries with difficult circumstances -- Angola, Ethiopia, Nigeria, and Zaire. The preliminary estimate of direct external and in-country costs averaged approximately 50[ per child vaccinated during the NIDs. Government in-kind contributions to NIDs, which were substantial in some countries, were not included in the cost calculations; therefore, the total cost per child vaccinated is an underestimate. Most external support was provided by Rotary International, UNICEF, WHO, and the U.S. government through the U.S. Agency for International Development and CDC. Cost data for SNIDs were not available. Reported by: Regional Office for Africa, World Health Organization, Brazzaville, Congo; Global Program on Vaccines and Immunization, World Health Organization, Geneva, Switzerland. Respiratory and Enterovirus Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: During 1996, NIDs were implemented in all countries in Europe and Asia where polio is endemic (2,3) and, for the first time, in many countries in the African Region. The initial experience with NIDs, conducted through the combined efforts of local and national governments and international partners, indicates that NIDs can be undertaken at modest costs in the African Region. Through the polio-eradication initiative, resources have been mobilized in support of enhanced planning, management, social mobilization, surveillance, and national and local political action for national vaccination programs (4,5). The strengthening of surveillance and other support systems is facilitating the development of the capacity for enhanced reduction of measles mortality; acceleration of neonatal tetanus elimination; and enhanced control of yellow fever, hepatitis B, epidemic meningitis, and other emerging or reemerging diseases (J.M. Okwo-Bele, Regional Office for Africa, World Health Organization, personal communication, 1997). Because population densities in Benin, Cameroon, Chad, Niger, and Nigeria and along the West African coast may form a geographically contiguous epidemiologic block, interruption of wild poliovirus transmission in this block is dependent on progress in vaccinating susceptible populations in each of these areas. Zaire also is important in polio-eradication efforts because wild polioviruses isolated during 1993-1995 in the surrounding countries of Angola, Namibia, Tanzania, and Zambia have been linked to earlier wild polioviruses isolated in Zaire (J.M. Okwo-Bele, Regional Office for Africa, World Health Organization, personal communication, 1997). Zaire, where polio is endemic, is the only country in the region that does not plan to conduct NIDs in 1997. Challenges in the African Region for 1997 are to ensure that all countries with endemic polio conduct NIDs (including those that experience internal strife and civil war), that routine vaccine coverage improves concurrently to approach or exceed the levels reported during the NIDs, and that sensitive surveillance systems for polio are implemented in all countries, including the approximately 4000 districts in the region. Surveillance for AFP and wild poliovirus will be used to monitor the progress in interrupting viral transmission and document the absence of wild poliovirus from the region and achieve polio eradication. The progress in the African Region suggests that, with continued efforts in implementing NIDs in all countries where polio is endemic, polio may be eradicated from the continent by the year 2000. References
* A confirmed case of polio is defined as acute flaccid paralysis and at least one of the following: 1) laboratory-confirmed wild poliovirus infection, 2) residual paralysis at 60 days, 3) death, or 4) no follow-up investigation at 60 days. ** Mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of prior vaccination history, with an interval of 4-6 weeks between doses. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Reported coverage with oral poliovirus vaccine during each round of
National Immunization Days (NIDs)* or Subnational Immunization Days (SNIDs),
by country -- African Region, World Health Organization, January 1996-March 1997
====================================================================================
Reported coverage (%) +
-----------------------------------
Supplemental activity/Country First round Second round
------------------------------------------------------------------------------------
NIDs
Algeria 89 90
Angola 71 80
Benin 103 91
Botswana 97 99
Burkina Faso 93 107
Cameroon NA & NA
Central African Republic @ NA NA
Chad ** 83 NA
Congo 82 91
C�te d'Ivoire 80 97
Equatorial Guinea 89 105
Eritrea 61 72
Ghana 90 96
Kenya 79 81
Lesotho 51 52
Malawi 74 86
Mauritania 89 95
Namibia 88 101
Nigeria 47 64
Rwanda 53 62
South Africa 90 77
Swaziland 82 85
Tanzania 97 102
Togo 83 96
Uganda 95 94
Zambia 87 88
Zimbabwe 96 96
SNIDs
Ethiopia 96 104
Gabon 78 82
Mozambique 81 81
Zaire 88 88
------------------------------------------------------------------------------------
* Mass campaigns over a short period (days to weeks) in which two doses of OPV are
administered to all children in the target age group, regardless of prior
vaccination history, with an interval of 4-6 weeks between doses.
+ Reported coverage may exceed 100% because of uncertainty about target population
(denominator problem) or vaccination of children outside the target age
(numerator problem).
& Not available.
@ The first round of NIDs was March 25-27, 1997, and data are incomplete.
** The first round of NIDs was March 3-8, and the second was March 31-April 5, 1997.
====================================================================================
Return to top. Figure_1 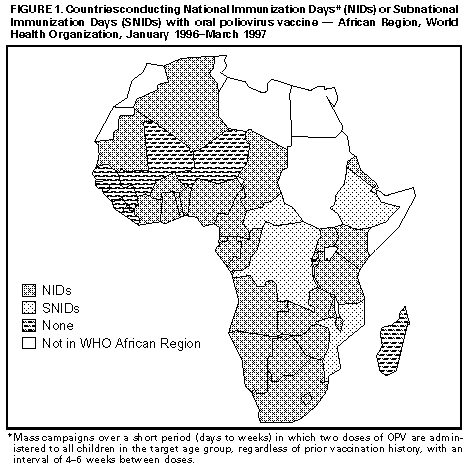 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}