 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Alcohol Consumption Among Pregnant and Childbearing-Aged Women -- United States, 1991 and 1995Moderate to heavy alcohol use by women during pregnancy has been associated with many severe adverse effects in their children, including fetal alcohol syndrome (FAS) -- with facial dysmorphology, growth retardation, and central nervous system deficits -- and other neurodevelopmental effects (1). Early prenatal alcohol exposure can occur unintentionally (i.e., before a woman knows she is pregnant); in addition, women who drink at high levels before pregnancy are at increased risk for drinking during pregnancy (2). Ongoing surveillance for alcohol consumption among pregnant and childbearing-aged women is important for monitoring the impact of efforts to prevent this risk behavior. This report analyzes and compares data from the 1995 Behavioral Risk Factor Surveillance System (BRFSS) and previously reported 1991 BRFSS data for women aged 18-44 years (3), and presents the prevalence of alcohol consumption among pregnant women and overall and state-specific prevalence rates among women of childbearing age. The findings indicate a substantial increase in alcohol use among pregnant women from 1991 to 1995. BRFSS is an ongoing, state-based, random-digit-dialed telephone survey of the U.S. civilian, noninstitutionalized population aged greater than or equal to 18 years. In 1995, all 50 states * participated in the BRFSS.** A total of 33,585 women aged 18-44 years were interviewed about their amount and frequency of alcohol consumption during the month preceding the survey. Based on their responses, drinking patterns were categorized as "any drinking" (consumption of at least one drink of alcohol during the preceding month) *** and as "frequent drinking" (consumption of an average of seven or more drinks per week or five or more drinks on at least one occasion). Data were weighted to reflect the probability of selection and state-specific postcensus population estimates by age, sex, and race, and standard errors were calculated by using SUDAAN. The small numbers of pregnant women sampled in each state preclude accurate state-specific prevalence rates for alcohol consumption among pregnant women. In 1995, 4.7% of women aged 18-44 years reported being pregnant at the time of the interview. Of these, 16.3% reported any drinking during the preceding month, compared with 12.4% in 1991 (p=0.07) (Table_1). The rate of frequent drinking among pregnant women was approximately four times higher in 1995 than in 1991 (3.5% in 1995 and 0.8% in 1991, p less than 0.01). This difference persisted after controlling for selected sociodemographic characteristics (i.e., age, household income, marital status, employment status, education level, smoking status, and race). Among all childbearing-aged women in 1995, 50.6% reported any drinking, and 12.6% reported frequent drinking -- prevalences similar to those in 1991 (49.4% reported any drinking, and 12.4% reported frequent drinking). The estimated state-specific prevalence of alcohol consumption among women aged 18-44 years varied substantially by state for both any drinking (from 26.1% in Utah to 68.2% in Wisconsin) and for frequent drinking (from 4.0% in Tennessee to 19.4% in Wisconsin) (Figure_1). For any drinking, rates were highest in Wisconsin, Massachusetts, Vermont, Rhode Island, and Connecticut. For frequent drinking, rates were highest in Wisconsin, Iowa, Pennsylvania, Minnesota, and Nevada. In general, in 1991 and 1995, prevalence rates of any and frequent drinking were highest in the northern regions. Reported by the following BRFSS coordinators: J Durham, MPA, Alabama; P Owen, Alaska; B Bender, Arizona; J Senner, PhD, Arkansas; B Davis, PhD, California; M Leff, MSPH, Colorado; M Adams, MPH, Connecticut; F Breukelman, Delaware; C Mitchell, District of Columbia; D McTague, MS, Florida; E Pledger, MPA, Georgia; J Cooper, MA, Hawaii; C Johnson, MPH, Idaho; B Steiner, MS, Illinois; N Costello, MPA, Indiana; P Busick, Iowa; M Perry, Kansas; K Asher, Kentucky; R Meriwether, MD, Louisiana; D Maines, Maine; A Weinstein, MA, Maryland; D Brooks, MPH, Massachusetts; H McGee, MPH, Michigan; N Salem, PhD, Minnesota; P Arbuthnot, Mississippi; T Murayi, PhD, Missouri; P Smith, Montana; S Huffman, Nebraska; E DeJan, MPH, Nevada; K Zaso, MPH, New Hampshire; G Boeselager, MS, New Jersey; W Honey, MPH, New Mexico; T Melnik, DrPH, New York; K Passaro, PhD, North Carolina; J Kaske, MPH, North Dakota; R Indian, MS, Ohio; N Hann, MPH, Oklahoma; J Grant-Worley, MS, Oregon; L Mann, Pennsylvania; J Hesser, PhD, Rhode Island; Y Gladman, South Carolina; M Gildemaster, South Dakota; D Ridings, Tennessee; K Condon, Texas; R Giles, Utah; R McIntyre, PhD, Vermont; L Redman, Virginia; K Wynkoop-Simmons, PhD, Washington; F King, West Virginia; E Cautley, MS, Wisconsin; M Futa, MA, Wyoming. Fetal Alcohol Syndrome Prevention Section, Developmental Disabilities Br, Div of Birth Defects and Developmental Disabilities, National Center for Environmental Health; Behavioral Risk Factor Surveillance Br, Office of Surveillance and Analysis, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial NoteEditorial Note: Official advisories warning against the use of alcohol by both pregnant women and women considering pregnancy were first released in 1981 (4) and again in 1990 (5) and 1995 (6). Although no safe level of alcohol consumption among pregnant women has been established, frequent consumption is associated with a greater risk for FAS and other neurodevelopmental effects (7,8). Despite the established health risk, substantial numbers of women continue to drink during pregnancy, and some at frequent levels. The BRFSS findings indicate that from 1991 to 1995, the prevalences of both any and frequent alcohol consumption by pregnant women increased substantially, even though the prevalences of these behaviors remained stable among all women aged 18-44 years. Alcohol consumption patterns in childbearing-aged women varied by geographic location; reasons for this variation may include age and sociocultural differences. The findings in this report are subject to at least four limitations. First, the percentage of women responding to BRFSS who reported they were pregnant was lower than other estimates (9) because BRFSS rates are point prevalence estimates, reflecting the status at the time of the interview rather than over an entire year. Second, BRFSS data were self-reported and may be subject to both recall and reporting biases. For example, because of the social stigmatization associated with heavy alcohol consumption, some women may underreport alcohol use. Third, because the question used to measure drinking status was modified from 1991 to 1995, the number of women with alcohol consumption categorized as any drinking possibly decreased in 1995 (women consuming less than one drink would have answered "yes" to the question in 1991 {any alcohol} but not in 1995 {at least one drink}). Finally, because the number of pregnant women in this sample who were drinkers was relatively small, the estimated prevalence rates are subject to both systematic biases and random variability. Despite these limitations, BRFSS is the largest ongoing population-based data source in the United States to include a representative sample of adult women and information on both alcohol consumption and pregnancy status. CDC will continue to use BRFSS to track alcohol-use patterns in pregnant women to assess public health efforts to reduce this risk behavior. Additional analyses of BRFSS data will include examining data from multiple years to further characterize trends and geographic differences in the drinking patterns of pregnant women and to identify risk factors associated with frequent alcohol use. Health-care professionals who provide care to women of childbearing age should inform their patients about the advisory on alcohol consumption, which recommends abstinence for women who are pregnant or planning to become pregnant. Because approximately half of the pregnancies in the United States are unintended (10), information about the effects of alcohol on the fetus should be provided to all childbearing-aged women who report frequent drinking. References
* For consistency over time, national analyses were restricted to the 47 states that participated in the BRFSS in both 1991 and 1995. State-specific analyses for 1995 included all 50 states. ** In analyzing the BRFSS, CDC used two methods of calculating response rates. The "upper bound" response rate is the ratio of completed interviews to the sum of all completed, refused, and terminated interviews. The Council of American Survey Research Organizations (CASRO) rate is more conservative, and follows a method developed by CASRO. This method factors in unanswered attempts and thus provides a measure of both telephone sampling efficiency and willingness to participate. For 1995, the median participant "upper bound" response rate was 80%, and the median CASRO response rate was 68%. *** In 1991, women were asked, "Have you had any beer, wine, wine coolers, cocktails, or liquor in the past month?" In 1995, women were asked, "During the past month, have you had at least one drink of any alcoholic beverages such as beer, wine, wine coolers, or liquor?" Other alcohol consumption questions did not change from 1991 to 1995. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Prevalence of reported alcohol consumption among pregnant and childbearing-aged women (18-44 years) -- United
States, Behavioral Risk Factor Surveillance System, 1991 and 1995 *
==========================================================================================================================================================
Pregnant women All women
----------------------------------------------------------- --------------------------------------------------------------
Reported 1991 1995 1991 1995
consumption level (n=1,053) (95% CI +) (n=1,313) (95% CI) p value (n=26,105) (95% CI) (n=30,415) (95% CI) p value
--------------------------------------------------------------------------------------------------------------------------------------------------------
Any drinking & 12.4 (9.5-15.2) 16.3 (13.1-19.4) 0.07 49.4 (48.4-50.3) 50.6 (49.7-51.6) 0.02
<7 Drinks per week 12.2 (9.4-15.0) 14.6 (11.5-17.6) 0.27 43.9 (43.0-44.9) 45.7 (44.8-46.5) 0.01
7-14 Drinks per week -- @ 0.9 ( 0.0- 1.8) -- 3.4 ( 3.1- 3.8) 3.0 ( 2.6- 3.3) 0.04
14 Drinks per week 0.1 (0.0- 0.3) 0.3 ( 0.0- 0.7) 0.28 1.4 ( 1.2- 1.6) 1.1 ( 0.9- 1.3) 0.04
>=5 Drinks on occasion ** 0.7 (0.2- 1.2) 2.9 ( 1.5- 4.3) 0.003 10.5 (10.0-11.1) 10.5 ( 9.9-11.1) 0.96
Frequent drinking ++ 0.8 (0.3- 1.4) 3.5 ( 1.9- 5.1) 0.002 12.4 (11.8-13.1) 12.6 (12.0-13.3) 0.67
--------------------------------------------------------------------------------------------------------------------------------------------------------
* Because weighted data are used in this analysis, results for 1991 may be slightly different from those reported previously. For
consistency, national analyses were restricted to the 47 states that participated in the BRFSS in both 1991 and 1995.
+ Confidence interval.
& Levels of any drinking may not add to the total prevalence of any drinking because some women did not respond to questions about
consumption frequency and amount. One additional state was eliminated from the breakdown of any drinking because questions
regarding consumption frequency and amount were not asked in that state in 1995.
@ Too few observations to calculate a reliable estimate.
** Five or more drinks on at least one occasion during the preceding month.
++ Consumption of an average of seven or more drinks per week or five or more drinks on at least one occasion during the preceding
month.
==========================================================================================================================================================
Return to top. Figure_1 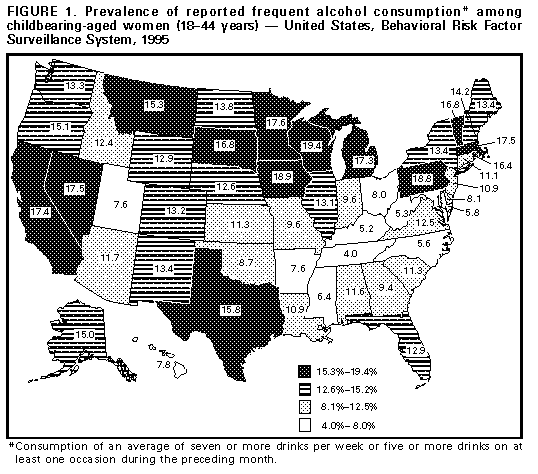 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}