 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
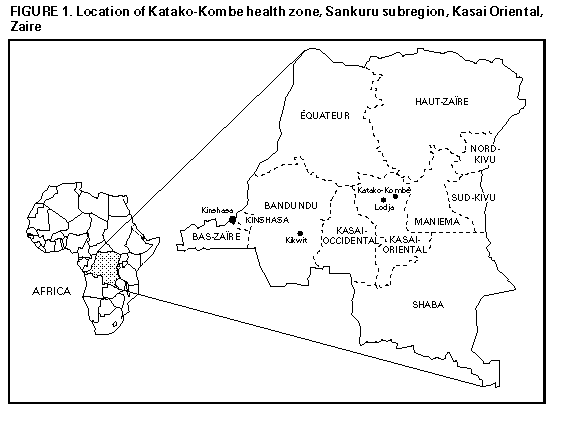
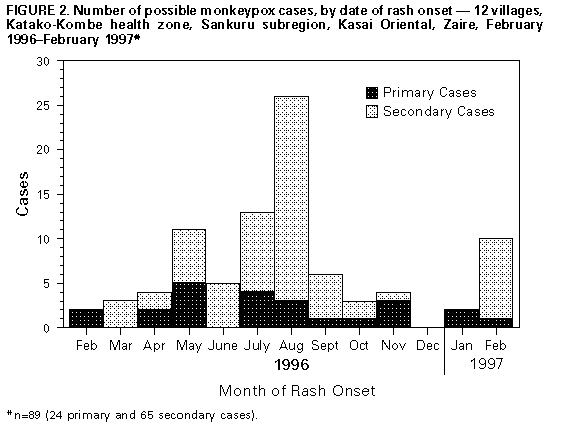
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Human Monkeypox -- Kasai Oriental, Zaire, 1996-1997Monkeypox is an orthopoxvirus with enzootic circulation in rainforests of central and western Africa; the virus can be transmitted to humans and cause a syndrome clinically similar to smallpox (e.g., pustular rash, fever, respiratory symptoms, and in some cases, death). From February through August 1996, a total of 71 clinical cases of monkeypox, including six deaths, occurred in 13 villages in Africa in the Katako-Kombe health zone (1996 combined population: 15,698), Sankuru subregion, Kasai Oriental, Zaire (Figure_1) (1). During the initial investigation of this cluster of human cases, specimens of serum and/or crusted scab or fluid from vesicles were collected from 11 patients, and monkeypox virus infection was confirmed in all 11 patients by the World Health Organization (WHO) Collaborating Center for Smallpox and Other Poxvirus Infections at CDC. Preliminary DNA phylogenetic studies of this strain of virus indicated only minor genetic variation compared with other strains of monkeypox virus from Zaire collected during 1970-1979. Because of reports by local public health officials of ongoing disease transmission, the Zaire Ministry of Health and WHO organized a follow-up investigation in February 1997 to characterize the magnitude of the outbreak. This report summarizes the preliminary results of the ongoing multidisciplinary investigation, which suggest that person-to-person transmission accounted for most monkeypox cases investigated in 1996 and 1997; in contrast, during previous years, reports were primarily for sporadic cases that resulted from animal-to-human transmission (2). As part of the follow-up investigation, during February 23-27, 1997, a dwelling-to-dwelling active case search was conducted in 12 villages (1997 combined population: 4057), including some of the villages in the initial investigation. A possible monkeypox case was defined as a vesicular, pustular, or crusted rash, not diagnosed as chickenpox by the family or the health-care provider, that occurred since January 1996 in a resident of the Katako-Kombe zone. A total of 92 possible monkeypox cases were identified (attack rate: 2%); seven cases had typical active vesiculo-pustular skin lesions. Fifty-one (55%) case-patients were male, and 25 (27%) were aged greater than or equal to 15 years. In Akungula, the village with the highest attack rate (11 per 100 population), the 45 reported cases were clustered in eight of the 44 housing compounds. Of the 84 case-patients for whom vaccination data were available, 15 (18%) had a vaccination scar on the upper left arm suggesting receipt of vaccinia vaccine; of these, 13 (87%) were aged greater than or equal to 25 years. Three (3%) of the 92 patients died; all were aged less than 3 years and died within 3 weeks of disease onset. The other three deaths reported during the initial investigation (1) either were not monkeypox cases or occurred in a village in which no active case search was conducted during the follow-up investigation. Of the 89 case-patients for whom data were available, 65 (73%) reported contact with another case-patient 7-21 days before onset of illness and thus were considered secondary cases. The number of possible cases identified per month increased during February-August 1996 and decreased gradually during subsequent months (Figure_2). However, in February 1997, the number of reported cases increased again. The number of secondary cases was highest in August 1996. Arboreal squirrels of the Funisciurus (Thomas' and Kuhl's tree squirrels) and Heliosciurus (sun squirrels) spp. have been implicated previously as probable reservoir hosts for monkeypox virus in Zaire based on antibody data and a single viral isolate from a Funisciurus anerythrus (2). In an attempt to assess the potential role of squirrels as a reservoir for monkeypox virus and to estimate the seroprevalence in wild-caught species, animals were hunted by local villagers and trapped by the study team. Over 4 days, 84 animals representing 16 species were captured; all animals were examined for lesions, and serum specimens were collected from 64 (76%). Except for one squirrel from which skin biopsies were collected, lesions suspected to be associated with monkeypox were not present on any other animals. Most of the animals captured and processed were Funisciurus sp. (22 {34%} of 64) and Cricetomys emini (Gambian rat) (15 {23%} of 64). Virus isolation and antibody studies are ongoing. Reported by: PT Mwamba, MD, KF Tshioko, MD, A Moudi, MD, World Health Organization-Zaire; V Mukinda, MD, Medecins Sans Fronti�res; GN Mwema, MD, D Messinger, National Institute of Biomedical Research; L Okito, MD, School of Public Health, Kinshasa, Zaire. D Barakymfyte, MD, African Regional Office, World Health Organization, Brazzaville, Congo. P Malfait, MD, R Pebody, MD, European Program for Intervention Epidemiology Training, Brussels, Belgium. M Szczeniowski, K Esteves, D Heymann, MD, Emerging and Other Communicable Diseases Surveillance and Control, World Health Organization, Geneva, Switzerland. Div of Applied Public Health Training (proposed), Epidemiology Program Office; Special Pathogens Br, and Poxvirus Section, Viral Exanthems and Herpesvirus Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Monkeypox virus, first identified in 1958 as a pathogen of cynomolgus monkeys, was associated with human illness in Zaire and West Africa during 1970-1971. The number of human monkeypox cases associated with the epidemic described in this report exceeded the total of 37 sporadic cases previously detected in the Sankuru subregion, Kasai Oriental region, by active surveillance activities during 1981-1986 (2). This outbreak was unrecognized until the end of July 1996, when an abrupt increase in the number of cases prompted a preliminary investigation by public health officials in Zaire (1). One person in a single village was the likely primary case-patient who may have been the source of infection for a cascade of person-to-person transmission to eight members of his family from February to July. During this period, monkeypox cases also were identified in persons who reported no contact with any other case-patient, suggesting introductions of monkeypox into the human population through contacts with wild animals. In a previous study (3), the low secondary attack rate of monkeypox within households suggested low potential for person-to-person transmission and inability of the infection to sustain itself in a human population. However, this outbreak -- with active cases continuing to occur in February 1997 -- differs from previously described monkeypox episodes. First, this outbreak represents the largest cluster of monkeypox cases ever reported. Second, the proportion of case-patients aged greater than or equal to 15 years (27%) was substantially higher than previously reported (8%) (2). Third, the proportion of secondary cases (73%) was substantially higher than previously reported (30%) (3). Fourth, the clustering of cases by household compounds and the previously undescribed prolonged chains of transmission suggest that person-to-person transmission accounted for most of the cases during this outbreak. Finally, the case-fatality proportion (3%) was lower than what was previously reported (10%). Cessation of vaccinia vaccination (which is protective against monkeypox infection) (2) in the late 1970s has resulted in an increase in the number of persons susceptible to monkeypox and could account for the magnitude of the outbreak and the higher proportion of case-patients aged less than 15 years. Local measures to interrupt disease transmission are ongoing and include education of health-care providers and distribution of health messages, such as limiting contact with wild-caught animals and restricting contact with suspected cases to a single person (preferably the oldest member of the household who has either recovered from monkeypox or has a vaccinia vaccination scar). Cohort studies of persons who had household or other close contact with monkeypox case-patients were interrupted during the investigation because of civil unrest in Zaire. These studies are needed to quantify the newly observed person-to-person transmission potential and to evaluate whether monkeypox infection can be sustained in a human population without the occurrence of new cases acquired through contact with wild animals. Analytical studies also should provide information about the natural history of monkeypox infection in humans and animals based on changing demographics and increased human interaction with the flora and fauna of the rainforest. The results of such studies will determine the need for additional risk-reduction measures, possibly including consideration of vaccinia vaccination under select circumstances. References
+-------------------------------------------------------------------
-------+
| Erratum: Vol. 46, No. 14
|
|
|
| In the article "Human Monkeypox -- Kasai Oriental, Zaire,
|
| 1996-1997," on page 307, in the last line of the first full
paragraph, |
| the age group is incorrect. The end of the sentence should read
|
| "... and the higher proportion of case-patients aged greater
than |
| 15 years."
|
+-------------------------------------------------------------------
-------+ Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}