 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Measles Outbreak -- Southwestern Utah, 1996During April 9-July 7, 1996, a total of 107 confirmed measles cases were reported from Washington County, Utah -- one of five counties in the Utah Southwest Health District (USHD). Fourteen cases associated with this outbreak were reported from other counties in Utah and from Arizona, California, and Nevada. This report summarizes the epidemiologic investigation of the outbreak in Washington County (1995 population: 65,885) and demonstrates the potential for measles to spread in a school-aged population despite a high coverage rate for at least one dose of measles vaccine. The index case was diagnosed in an unvaccinated 17-year-old high school student on April 10 (Figure_1). By April 25, seven additional cases had been reported from the same school. During April 26-July 1, a total of 99 additional cases were reported from Washington County. The source of infection for the index case could not be identified. Case-patients ranged in age from 6 months to 45 years (median: 14 years). Sixty-six (62%) cases occurred among children in grades 5-12, and four (4%) cases (including three in persons with philosophic objections to vaccination) occurred among children in grades K-4 (Figure_2). Six (6%) cases occurred among infants (aged less than 12 months) who were too young to have received measles vaccination (1). Of the 99 case-patients eligible for measles vaccination *, 64 (64%) had not been vaccinated, 34 (34%) had received one dose of a measles-containing vaccine (MCV), and one (1%) had received two doses of an MCV. From 1975 to 1992, Utah required documentation of receipt of one dose of an MCV for every child entering kindergarten or first grade; since 1992, two doses have been required. Children in grades K-4 at the time of the outbreak were covered by the requirement for two doses, and children in grades 5-12 were covered by the one-dose requirement. However, exemptions for medical, philosophic, or religious reasons are permitted. Probable sites of exposure to measles for confirmed cases were schools (59 cases) and day care centers (five cases), home (27 cases), and other settings (11 cases); the probable site of exposure was unknown for five cases. No deaths, hospitalizations, or other major complications were reported among the case-patients in this outbreak. A vaccine effectiveness study was conducted at the high school where the outbreak was initially reported. Review of school vaccination records of the 879 students attending the school at the time of the outbreak indicated that 780 (89%) students had received one dose of measles-mumps-rubella vaccine (MMR), 72 (8%) had received two doses of MMR, and 27 (3%) were unvaccinated. Seventeen unvaccinated students had philosophic exemptions, and 10 had no record of measles vaccination in their school health files. The measles attack rate among unvaccinated students was 33% (nine cases) and among recipients of one dose of MMR was 1% (eight cases). No cases of measles were diagnosed among any of the recipients of two doses of MMR in this high school. Vaccine effectiveness (VE) was calculated using the following formula: VE (%)={(ARU - ARV) / ARU} X 100, where ARU is the attack rate for the unvaccinated students and ARV is the attack rate for the vaccinated students (2). Based on this approach, VE was estimated to be 97% among students with a documented history of receipt of one dose of MMR vaccine and 100% in students with two doses of MMR. Three control measures were instituted to prevent spread of the outbreak. First, because cases were occurring among infants, the age for vaccination eligibility was lowered to 6 months. Second, children in Washington County for whom proof of vaccination or immunity could not be established were excluded from schools and day care centers. Third, a mass vaccination campaign was initiated on June 10. Approximately 20,000 doses of MMR were administered throughout the USHD (with almost 90% of doses administered in Washington County). Among 10,800 children in grades 5-12 in Washington County, an estimated 56% received one dose of MMR during the vaccination campaign. Two-dose MMR vaccination coverage among children in grades 5-12 is estimated to have improved from 10% before the campaign to 65%. Reported by: GL Edwards, MS, S Finch, R Adams, Southwest Utah Public Health Dept, St. George; R Crankshaw, R Ward, F Alvarez, P Weatherhogg, MSW, Immunization Program, Div of Maternal and Child Health, CR Nichols, MPA, State Epidemiologist, Utah Dept of Health. Assessment Br, Data Management Div; Measles Elimination Activity, Child Vaccine Preventable Disease Br, Epidemiology and Surveillance Div; and Program Operations Br, Immunization Svcs Div, National Immunization Program; Measles Virus Section, Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: The measles outbreak in southwestern Utah was the largest such outbreak in the United States in 1996 and accounted for approximately 25% of all measles cases reported to CDC during 1996 (3). The next largest outbreak in 1996, which occurred in Juneau, Alaska, included 63 cases and affected school-aged children who had not received two doses of an MCV (4). The outbreak in Utah began in a high school in which most (97%) students had previously received at least one dose of an MCV and only a small percentage (8%) had received two doses. Measles outbreaks in schools with high one-dose coverage with a highly effective vaccine highlight the contagiousness of measles and the necessity for routine vaccination with two doses of an MCV (5,6). In Utah, the school requirement for two doses of an MCV covered grades K-4 and probably prevented measles transmission among children in those grades. The potential impact of a second dose of an MCV is illustrated by the occurrence of only one case among recipients of two doses in the Utah outbreak and the estimated 100% vaccine effectiveness among two-dose recipients in the high school based on the vaccine effectiveness study. The vaccination campaign in southwestern Utah rapidly improved two-dose MMR coverage and may have helped to control the outbreak. During measles outbreaks in schools, coverage with two doses of MMR should be accelerated in school populations. The national goal for measles vaccination is that all school-aged children will have received two doses of an MCV by 2001 (7). In June 1997, the Vaccines for Children (VFC) program, a national program making federally purchased vaccines available at no cost to health-care providers for administration to eligible children, began covering the cost of a second dose of MMR for VFC-eligible children in every grade. Full coverage with the second dose of MMR for all schoolchildren is needed to assure the elimination of measles in the United States. References
* Persons aged greater than or equal to 12 months born during or after 1957. Figure_1 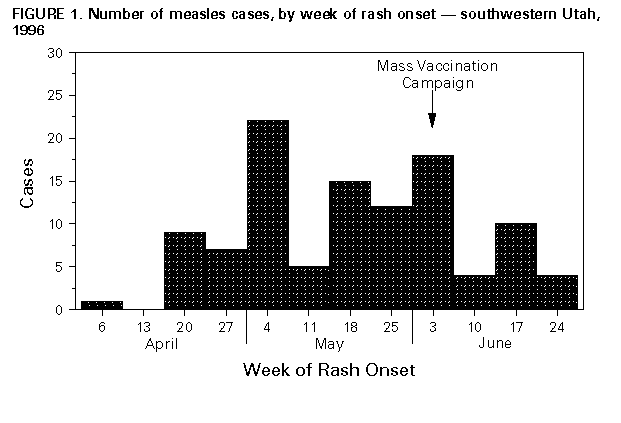 Return to top. Figure_2 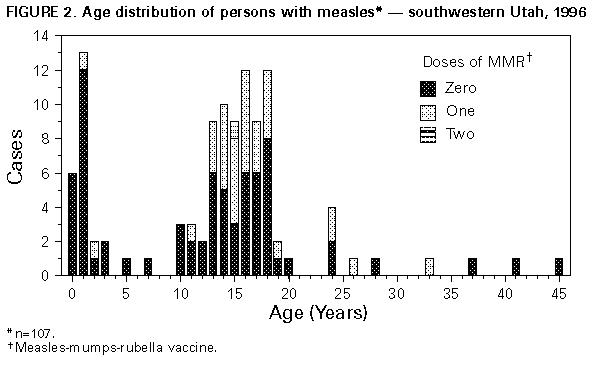 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}