 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Influenza Activity -- United States, 1997-98 SeasonIn collaboration with the World Health Organization (WHO), its collaborating laboratories, and state and local health departments, CDC conducts surveillance to monitor influenza activity and to detect antigenic changes in the circulating strains of influenza viruses. This report summarizes influenza surveillance in the United States from September 28, 1997, to January 10, 1998, which indicates that influenza activity, predominantly attributable to influenza A(H3N2) viruses, increased from mid-December through early January, and two antigenically related but distinguishable strains of influenza A(H3N2) viruses, A/Nanchang/933/95-like and A/Sydney/05/97-like, have been identified. Few influenza B isolates have been identified. The number of influenza isolates identified by WHO collaborating laboratories and the percentage of respiratory specimens positive for influenza increased each week from December through early January. From September 28 through January 10, WHO collaborating laboratories tested 21,770 respiratory specimens, and 985 (4.5%) were positive for influenza. Of the 985 influenza isolates, 981 (99.6%) were influenza A, and four (0.4%) were influenza B. All of the 250 influenza A isolates that have been subtyped are A(H3N2). Of the 43 influenza A(H3N2) viruses collected since September 28 that have been antigenically characterized by CDC, 26 (60%) are similar to A/Nanchang/933/95, the A/Wuhan/359/95(H3N2)-like strain used by U.S. manufacturers in the 1997-98 influenza vaccine; the remaining 17 (40%) are similar to A/Sydney/05/97, a related but antigenically distinguishable variant. A/Nanchang/933/95-like isolates were identified from 11 states (Alaska, Arizona, California, Hawaii, Louisiana, Missouri, New York, Pennsylvania, Texas, Washington, and Wisconsin), and A/Sydney/05/97-like viruses were identified from eight states (California, Florida, Hawaii, Louisiana, Minnesota, New York, Texas, and Wisconsin). Although the number of isolates characterized is small, the proportion of A/Sydney/05/97-like viruses increased each month since September 28. One influenza B isolate has been submitted to CDC for antigenic characterization, and it is similar to the vaccine strain B/Harbin/07/94. For the week ending January 10 (week 1), state and territorial epidemiologists reported widespread or regional activity* in 26 states (Figure_1) compared with 15 states for week 53 and 10 states for week 52. Most laboratory-confirmed influenza outbreaks reported by states to CDC have occurred among nursing-home residents, although some reported outbreaks have been among children and young adults. Although the percentage of patient visits to sentinel physicians for influenza-like illness (ILI) has exceeded baseline levels (0-3%) for at least 1 week in five of nine regions (Mid-Atlantic, South Atlantic, West South Central, Mountain, and Pacific), for the United States as a whole, the level of ILI has not exceeded baseline levels this season. The percentage of deaths attributed to pneumonia and influenza as reported by the vital statistics offices of 122 cities exceeded the epidemic threshold of 7.2% for the week ending January 10 (week
Reported by: Participating state and territorial epidemiologists and state public health laboratory directors. World Health Organization collaborating laboratories. WHO Collaborating Center for Surveillance, Epidemiology, and Control of Influenza, Influenza Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC. Editorial NoteEditorial Note: Influenza activity in the United States increased from December through early January, and influenza A(H3N2) viruses have been most commonly isolated. Since the emergence of influenza A(H3N2) viruses in 1968, seasons during which these viruses predominate typically have been associated with higher morbidity and mortality, particularly among the elderly, than have seasons during which influenza A(H1N1) or influenza type B viruses predominated (1). A/Sydney/05/97(H3N2)-like viruses, which were first identified in New Zealand and Australia during June 1997, are related but antigenically distinguishable from A/Nanchang/933/95, the H3N2 component of the 1997-98 influenza vaccine. Antibodies produced against the A/Nanchang/933/95(H3N2) component of the vaccine do cross-react with A/Sydney/05/97-like viruses (2). However, because vaccine effectiveness is dependant, in part, on the match between the vaccine and the circulating strains, vaccine efficacy might be decreased in persons infected with A/Sydney/05/97-like viruses. The current co-circulation of two influenza A(H3N2) strains emphasizes the importance of timely submission of influenza isolates for antigenic characterization by state public health laboratories and WHO collaborating laboratories. Even when the match between circulating strains and the vaccine strain is good, outbreaks of influenza can still occur among vaccinated persons. Therefore, use of the antiviral agents amantadine and rimantadine is an important measure in the prevention and control of influenza type A, particularly for persons at high risk for influenza-related complications. During an institutional outbreak of influenza A, facilities (e.g., nursing homes) that house persons at increased risk for influenza-related complications should consider using amantadine or rimantadine for prophylaxis and/or treatment (3). These drugs are 70%-90% effective in preventing influenza A infections and can reduce the severity and duration of symptoms from influenza A when administered within 48 hours of illness onset. Rapid diagnosis of influenza type A infection is valuable for early detection of outbreaks and selection of appropriate treatment because neither drug is effective against influenza type B viruses. Throughout the season, influenza surveillance data are updated weekly and are available through CDC's fax information system, telephone (888) 232-3299 ({888} CDC-FAXX) by requesting document number 361100 and entering the telephone number to which the document should be transmitted, or through CDC's National Center for Infectious Diseases, Division of Viral and Rickettsial Diseases, Influenza Branch World-Wide Web site http://www.cdc.gov/ncidod/diseases/flu/weekly.htm. References
* Levels of activity are 1) no activity; 2) sporadic -- sporadically occurring influenza-like illness (ILI) or culture-confirmed influenza, with no outbreaks detected; 3) regional -- outbreaks of ILI or culture-confirmed influenza in counties with a combined population of less than 50% of the state's total population; and 4) widespread -- outbreaks of ILI or culture-confirmed influenza in counties with a combined population of greater than or equal to 50% of the state's total population. Figure_1 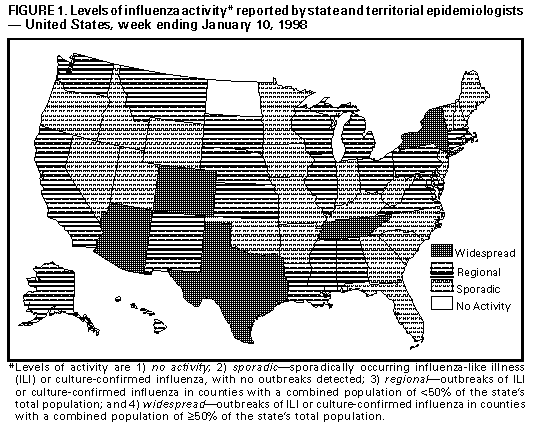 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}