 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Suicide Prevention Evaluation in a Western Athabaskan American Indian Tribe -- New Mexico, 1988-1997Since 1979, suicide and homicide have alternated as the second and third leading causes of death * among young American Indians and Alaska Natives (AI/ANs). From 1979 through 1992, suicide rates for AI/ANs in all age groups were approximately 1.5 times the rates for the overall U.S. population. During 1991-1993, suicide rates for AI/ANs aged 15-24 and 25-34 years were 31.7 and 26.6 per 100,000 population, respectively; males aged 15-34 years accounted for 64% of all AI/AN suicides (1). In the overall U.S. population during 1991-1993, the rates for persons in these same age groups were 13.0 and 14.5, respectively (2). Since 1980, suicide has been either the second or third leading cause of death for persons aged 15-24 years in the overall U.S. population (3). Although knowledge about suicide among AI/ANs has increased (4), information about the efficacy of suicide prevention and intervention programs in general, and specifically in AI/AN communities, is scarce. In January 1990, following concern raised by tribal officials in 1988 about suicide among youth, a Western Athabaskan tribe in rural New Mexico implemented a suicide prevention and intervention program that targeted tribal members aged 15-19 years (5,6). This report summarizes the results of the program through 1997 and indicates that rates of suicide and attempted suicide among this target population decreased substantially after the program was implemented. From 1988 to 1997, the tribal population increased from 2762 to 3225. The population of tribal members aged 15-19 years increased similarly, from 283 to 328. Ninety percent of the population lived on the reservation, primarily in the one reservation town. Approximately 80% of persons aged greater than or equal to 16 years were unemployed, with some seasonal variation (Western Athabaskan Tribe, unpublished data, 1998). The prevention and intervention program included previously unavailable services for the entire community. CDC guidelines for containing suicide clusters (7) and developing suicide prevention programs among adolescents and young adults (8) were incorporated into program activities. School-based "natural helpers," comprising 10-25 youth per year, were trained to respond to young persons in crisis and to notify mental health professionals of the need for assistance. Natural helpers also provided education in both the school and community on alcohol and drug prevention, self-esteem and team building, and suicide prevention. Prevention of alcohol abuse, child abuse, and violence between intimate partners was included in the program because these behaviors have been associated with suicidal behavior (4). Other program components included outreach to families after a suicide or traumatic death or injury, immediate response and follow-up for reported at-risk youth, community education about suicide prevention, and suicide-risk screening in mental health and social service programs. A surveillance form developed by IHS in 1988 was revised and used by local professional staff to collect information about suicide completions and attempts. Attempts included both self-inflicted injuries requiring medical or other intervention to prevent death and injuries that may have required medical intervention but were not potentially lethal. Program staff assessed all persons who made suicide attempts. Information about suicide completions was obtained from police records, health clinic records, tribal emergency medical services records, and family and community members. Rates of suicidal acts before and after program implementation for persons aged 15-19 years were compared to assess program effectiveness. Demographic information obtained about persons who committed a suicidal act included age, sex, marital status, tribe, employment, education, and living arrangements. Other pertinent information collected included method used, number of previous suicidal acts, location of suicidal act, alcohol and/or substance abuse, family history of suicidal behaviors, loss of job, break-up with or death of a significant other, and suicide of a friend. During 1988-1997, a total of 118 persons in all age groups accounted for 237 suicidal acts (i.e., all suicide completions and attempts). Sixty-four (54.2%) of these persons had previously exhibited suicidal behaviors; 165 (69.6%) of all acts involved alcohol use. Of all suicidal acts, 15 (6.3%) resulted in death; all suicide completions were among males. The ratio of suicidal attempts to suicidal completions was 14.8:1. Males accounted for more attempts than females (114 males, 108 females). Of all these suicidal acts, 61 (25.7%) occurred among persons aged 15-19 years. Rates of suicidal acts for persons aged 15-19 years and for all other age groups were calculated in 2-year intervals for rate stability (Figure_1). The numbers of suicide completions were too small to calculate separate rates by age group. During 1988-1989 (i.e., before program implementation), the suicidal act rate for persons aged 15-19 years was 59.8 (n=34) per 1000 population, compared with 7.5 (n=38) per 1000 for all other age groups. During 1990-1991, the rate for persons aged 15-19 years decreased to 8.9 (n=5) per 1000 population. This rate increased slightly to 9.2 (n=5) during 1992-1993, rose to 17.6 (n=10) during 1994-1995, and decreased to 10.9 (n=7) during 1996-1997. Although rates varied after implementation of the program, they remained substantially lower than before the program was initiated. During these same time periods, rates for all other age groups demonstrated considerably less variation. Reported by: Western Athabaskan Tribe. P Serna, MSW, American Indian/Alaska Native Suicide Prevention Center and Network; PA May, PhD, Univ of New Mexico, Albuquerque, New Mexico. M Sitaker, MPH, Office of Epidemiology and Assessment, The Combined Health District of Montgomery County, Dayton, Ohio. Indian Health Service, Albuquerque, New Mexico. Div of Violence Prevention, National Center for Injury Prevention and Control, CDC. Editorial NoteEditorial Note: Since this program was implemented in 1990, rates of suicidal acts substantially decreased for members of the Western Athabaskan tribe aged 15-19 years. Aspects of the program that possibly contributed to the decrease in rates included multiple prevention and intervention strategies within a centralized population and full-time program staff dedicated to suicide prevention and intervention. A decrease in suicidal behaviors coincident with community education and heightened screening suggests an actual program effect. This decrease in suicidal behaviors occurred despite consistent surveillance and heightened community education about suicide prevention. The results of the program evaluation are subject to three limitations. First, the program was not implemented simultaneously in a comparison group or population, which made determination of program effectiveness difficult. Second, it could not be determined which program prevention components were associated with the reduction in suicidal acts. Finally, during 1958-1987, Athabaskan tribes in New Mexico demonstrated a cyclical increase and decrease in the rate of suicide completions every 5-6 years (9). An analysis of suicide prevalence rates since 1987 for other Athabaskan tribes in New Mexico will be necessary to compare populations who have not implemented suicide prevention activities and to determine 1) whether cyclical patterns of suicide completions have continued in Athabaskan tribes, 2) whether the suicide prevention program was implemented during a downward cycle or has had the suggested impact in reducing suicidal behaviors, and 3) whether patterns of suicide completions (i.e., excluding nonfatal suicidal acts) adequately measure the success of local prevention programs. Additional research is needed to determine both risk and protective factors for suicide and the reasons for higher suicide rates in some AI/AN communities. Sociocultural factors that might be involved include the availability of employment and educational opportunities, the role of alcohol in AI/AN communities, community history of suicidal behavior, and loss or maintenance of traditional spiritual practices and indigenous languages. During 1993-1994, suicide prevention activities in this community were expanded to include persons aged 20-24 years. Further evaluation will be necessary to determine the effect of the program on persons in this age group. CDC guidelines for prevention of suicide among adolescents and young adults suggest avoiding reliance on any one strategy (8). Additional investigation is necessary to determine which strategies are most effective in preventing suicidal behavior among AI/ANs. The suicide prevention program in this American Indian community underscores the value of consistent surveillance to track trends in suicidal behaviors and assess program effects. Replication and evaluation of similar programs are needed to further develop effective suicide prevention strategies for adolescents and young adults. References
* The leading cause of death has been injury resulting from motor-vehicle crashes. Figure_1 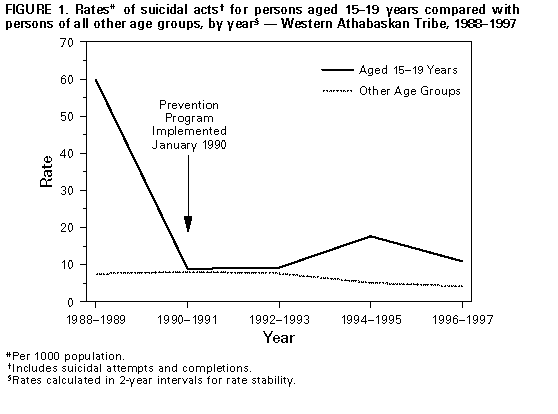 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}