 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Measles -- United States, 1997During 1997, a provisional total of 138 confirmed measles cases was reported to CDC by local and state health departments, the lowest number of measles cases ever reported in 1 year and a 55% decrease from the previous record low of 309 cases reported in 1995 (Figure_1). This report describes the epidemiology of measles in the United States in 1997, which suggests that no endemic measles virus is circulating in the United States. Case Classification Reported measles cases are classified as imported or indigenous based on where transmission of measles virus is likely to have occurred. Cases in persons who traveled outside the United States within 18 days before rash onset are classified as international importations. Indigenous measles cases are classified into three groups: 1) cases linked epidemiologically to a known international importation, 2) cases in which a measles virus strain is isolated that has been associated with other countries (1), and 3) all other cases in which no association to an importation was detected. Of the 138 cases reported in 1997, a total of 57 (41%) were international importations. Thirty-six (63%) occurred in visitors traveling to the United States from other countries. The remaining 21 imported cases occurred in U.S. residents who were abroad during the exposure period. The countries from which measles was most frequently imported were Germany (nine cases), Italy (nine), Switzerland (five), Brazil (five), and Japan (four). Of the 81 indigenous cases, 17 (21%) cases were linked epidemiologically to international importations. The maximum number of cases epidemiologically linked to a single imported case was four. The longest reported chain of measles transmission following an imported case lasted 5 weeks. Measles virus was isolated from two chains of transmission that included seven (9%) of the 81 indigenous cases; the isolated measles strains have been associated with disease in other countries (1). There was no epidemiologic link or virologic evidence suggesting importation for the remaining 57 (70%) of the 81 indigenous cases. In 1997, there was epidemiologic or virologic evidence of an international source for 81 (59%) of the 138 cases reported to CDC, compared with 15% in 1995 and 28% in 1996. Geographic Distribution In 21 states, no measles cases were reported for 1997, and in 20 states and the District of Columbia, fewer than five cases were reported. Nine states (Arizona, California, Florida, Massachusetts, Minnesota, New York, Pennsylvania, South Dakota, and Texas) accounted for 64% of total cases and 56% of imported cases. Temporal Patterns of Transmission The maximum number of reported cases occurring in a single week was 11, and the median number of cases per week was two. In 9 weeks, no reported cases occurred, and in 21 weeks, all reported cases were associated with imported cases (Figure_2). Age and Vaccination Status The predominant age groups with confirmed measles were preschool-aged children (1-4 years) (40 {29%} cases), followed by persons aged 5-19 years (39 {28%} cases), and persons aged 20-39 years (36 {26%} cases). Of the 138 patients, 32 (23%) had a documented history of vaccination with measles-containing vaccine (MCV): 25 (18%) patients had received one dose of MCV, and seven (5%) had received two doses of MCV. The remaining 106 (77%) patients reported being unvaccinated. For all persons with reported measles in age groups for which vaccine is recommended, 62% were unvaccinated. Outbreaks A total of 13 outbreaks, defined as three or more epidemiologically linked cases, were reported to CDC by 11 states. Outbreak-related cases accounted for 44% of all cases. The largest outbreak involved eight cases (median: four; range: three to eight cases). Adult/postschool-related and preschool-related outbreaks were the most common, with four outbreaks each, and three outbreaks involved persons with philosophic or religious objections to vaccination. One school-related and one college-related outbreak also were reported. Five (38%) of the 13 outbreaks had known international sources. Reported by: State and local health depts. Measles Virus Section, Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Measles Elimination Activity, Child Vaccine Preventable Disease Br, Epidemiology and Surveillance Div, National Immunization Program, CDC. Editorial NoteEditorial Note: The 138 confirmed measles cases in 1997 represent a record low since measles became a nationally reportable disease in 1912. Since the 1989-1991 measles resurgence, the number of reported measles cases has declined substantially, with record low numbers reported during 1993-1997 and less than 500 cases reported during 1993, 1995, and 1997. The isolated geographic distribution of measles cases, the small number of reported measles cases, and the lack of a recurrent viral strain suggest that there is no endemic circulation of measles virus in the United States (1). The current pattern of reported measles cases suggests continual importations of measles virus resulting in short chains of secondary transmission in the United States. Some of the indigenous cases that were not associated with importation may have resulted from incomplete reporting and undetected transmission in these chains. Others may have been associated with exposure to undetected importations, or may have been misclassified resulting from false-positive laboratory tests. Limited secondary transmission following international importation demonstrates the success of vaccination efforts in the United States in increasing population immunity. The measles vaccine coverage rate among children aged 19-35 months was 91% in 1996 (2), and second-dose coverage is increasing among school children through expanding implementation of school requirements for two doses of measles vaccine. However, there are still groups in the population with low measles immunity. The groups most likely to be vulnerable to measles include those with religious or philosophic objections to vaccination, students in grades not required to have two doses of measles vaccine, health-care workers, and preschool-aged children in areas with low vaccination coverage (3,4). The exposure of such groups to an imported case could result in large outbreaks. Continued promotion of vaccination, better implementation of the two-dose vaccination requirement, and improved vaccination of health-care workers should decrease the risk for potential outbreaks among these groups. Permanent elimination of indigenous transmission of measles in the United States will require strong surveillance and high levels of population immunity. Cooperation with other countries to enhance control of measles can reduce the burden of measles in those countries and the risk for importations to the United States. The decrease in importations to the United States from other countries in the Americas following measles elimination efforts underscores the benefits of coordinated measles elimination efforts in the region (5). For example, only five importations from elsewhere in the Americas were detected in 1997 (compared with 242 cases in 1990) after increased efforts in measles control (6). The Pan American Health Organization established the goal of eliminating measles from the Western Hemisphere by 2000, and the Eastern Mediterranean Regional Office of the World Health Organization (WHO) established a regional goal of measles elimination by 2010. The European Regional Office of WHO is considering establishing a measles elimination goal. Elimination of measles from other regions of the world greatly reduces the risk for importation and spread of measles in the United States. The goal of global elimination is being considered but has not yet been established. References
Figure_1 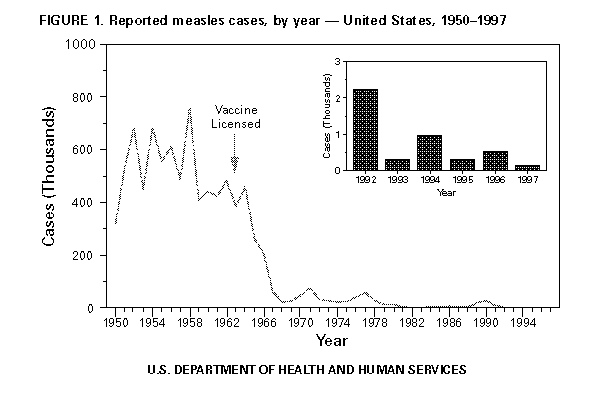 Return to top. Figure_2 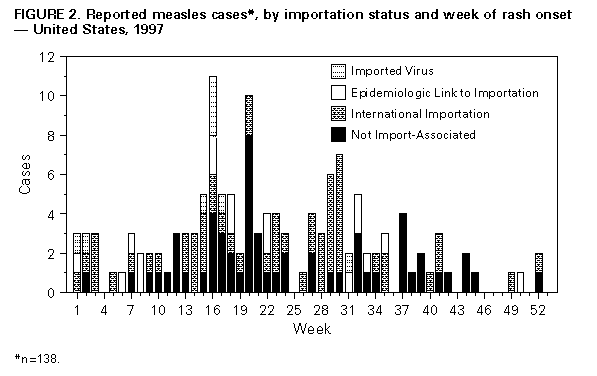 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}