 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Heat-Related Mortality -- United States, 1997Environmental heat exposure can cause illness, injury, and death. This report describes four heat-related deaths that occurred in the United States during 1997 and summarizes risk factors for and reviews measures to prevent heat-related illness, injury, and death. Case 1. On June 18, in New York City, a previously healthy 61-year-old woman was found dead in a sauna of an apartment building. The sauna room temperature was 90 F (32.2 C). The sauna did not have a timer. Her blood alcohol level was 0.21% (New York State's legal limit is 0.10%). The cause of death was heat exposure associated with acute alcohol intoxication. Case 2. On July 4, in Oakland County, Michigan, a previously healthy but overweight 14-year-old male was found dead in his home. He had been lifting weights and was wearing only shorts. The outdoor air temperature was 74 F (23.3 C), but the heat was on in the home with the temperature set at 85 F (29.4 C). He had begun a program of lifting weights 2 week before his death. The toxicology report from the autopsy detected no drugs in his serum or urine. The cause of death was acute congestive heart failure caused by strenuous weight lifting and heat exhaustion. Case 3. On July 18, in New York City, a 37-year-old man was found dead at a transition house for homeless persons with mental illness. During July 17-18, a power failure had occurred in the house, and the ambient temperature was greater than 90 F (greater than 32.2 C). Two days before the power outage, he had complained of influenza-like symptoms. He was taking several medications, including amantadine, lithium, and lorazepam. He died from hyperthermia complicated by lithium therapy for bipolar disorder. Case 4. On August 5, in Los Angeles, a 47-year-old woman collapsed in her residence, which was not air-conditioned. Paramedics transported her to the hospital, where she was pronounced dead. She had a history of hypertension and weighed approximately 300 lbs; the medical report noted no obvious trauma. The outdoor temperature was at least 100 F (37.8 C). The cause of death was listed as hyperthermia. Reported by: DR Schomburg, Chief Medical Examiner's Office, New York City; L Berenson, Office of Vital Statistics and Epidemiology, New York City Dept of Health. L Dragovic, MD, Oakland County Medical Examiner's Office, Oakland County, Michigan. L Sathyabagiswaran, Chief Medical Examiner's Office, S Ahonima, County of Los Angeles, Los Angeles, California. Health Studies Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; and an EIS Officer, CDC. Editorial NoteEditorial Note: During 1979-1995, a total of 6615 deaths in the United States were attributed to excessive heat exposure *; of these, 2792 (42%) were "due to weather conditions"; 327 (5%) were "of man-made origin"; and 3496 (53%) were "of unspecified origin." Of the 2744 persons for whom age data were available, persons aged greater than or equal to 55 years accounted for 1692 (62%), and children aged less than or equal to 14 years accounted for 109 (4%) heat-related deaths "due to weather conditions." Except for children aged less than or equal to 14 years, the average annual rate of heat-related deaths increased with each age group, particularly for persons aged greater than or equal to 55 years (Figure_1). Because other causes of death (e.g., cardiovascular and respiratory diseases) also increase during heat waves (1,2), heat-related deaths "due to weather conditions" represent only a portion of heat-related excess mortality. The criteria to define a heat-related death differ by state and among individual medical examiners and coroners (3-5). The National Association of Medical Examiners defines heat-related death as exposure to high ambient temperature either causing the death or substantially contributing to the death (3). The cases described in this report highlight risk factors for heat-related death: alcohol consumption, overweight, use of some medications (e.g., neuroleptics and tricyclic antidepressants), and physical activity (e.g., exertion in unusually hot environments) (1,4,6). Other factors associated with increased risk for heat-related illness and death include age (e.g., the very young and the elderly), history of previous heatstroke, chronic conditions (e.g., cardiovascular or respiratory diseases), social circumstance (e.g., living alone), and physical or mental impairment or bed confinement that interferes with ability to care for oneself or to avoid hot environments (1,4,6). However, all persons can be at risk if exposed to excessive heat (4). Adverse health conditions associated with high environmental temperatures include heatstroke, heat exhaustion, heat syncope, and heat cramps (4). Heatstroke is a medical emergency characterized by rapid onset and progression (within minutes) of the core body temperature to greater than or equal to 105 F (greater than or equal to 40.6 C) and lethargy, disorientation, delirium, and coma (4). Heatstroke is often fatal despite expert medical care directed at rapidly lowering the body temperature (e.g., ice baths) (4). Heat exhaustion is characterized by dizziness, weakness, or fatigue often following several days of sustained exposure to hot temperatures and results from dehydration or electrolyte imbalance (4); treatment for heat exhaustion is directed at replacing fluids and electrolytes and may require hospitalization (4). Hot weather and standing or mild exercise may increase the likelihood of heat syncope and heat cramps caused by peripheral vasodilation. Treatment of persons with loss of consciousness as a result of heat syncope should include placement in a recumbent position with feet elevated and electrolyte replacement (4). Persons working in high temperatures -- either indoors or outdoors -- should take special precautions, including allowing 10-14 days to acclimate to an environment of high ambient temperature. Adequate salt intake with meals is important; however, salt tablets are not recommended and may be hazardous (4). Although using fans can increase comfort at temperatures less than 90 F (less than 32.2 C), fans are not protective against heat-related illness when temperatures are greater than or equal to 90 F (greater than or equal to 32.2 C) and humidity greater than 35% (1,7). Strategies for preventing heat-related illness during exercise or because of human causes (e.g., saunas) include acclimating to the climate and consulting a health-care professional to develop an exercise regimen (8,9). Other strategies include increasing time in air-conditioned environments, increasing nonalcoholic fluid intake, exercising only during cooler parts of the day, and taking cool-water baths (1). Persons whose fluid consumption is restricted for medical reasons should consult their physician before altering their fluid intake (4). Elderly persons should be encouraged to take advantage of air-conditioned environments (e.g., shopping malls and public libraries), even if only for part of the day (1,4,6). Public health information about exceptionally high temperatures should be directed toward susceptible populations. For example, parents should be educated about the higher sensitivity to heat of children aged less than 5 years (4). When a heat wave is predicted, prevention messages about avoiding heat-related illness should be disseminated to the public as early as possible to prevent heat-related illness, injury, and death (5). References
* Underlying cause of death attributed to excessive heat exposure, classified according to the International Classification of Diseases, Ninth Revision (ICD-9), as E900.0, "due to weather conditions"; E900.1, "of man-made origin"; or E900.9, "of unspecified origin." These data were obtained from the Compressed Mortality File, provided by CDC's National Center for Health Statistics. It contains information from death certificates filed in the 50 states and the District of Columbia through the National Vital Statistics System. Cause of death has been coded in accordance with the provisions of ICD-9. Figure_1 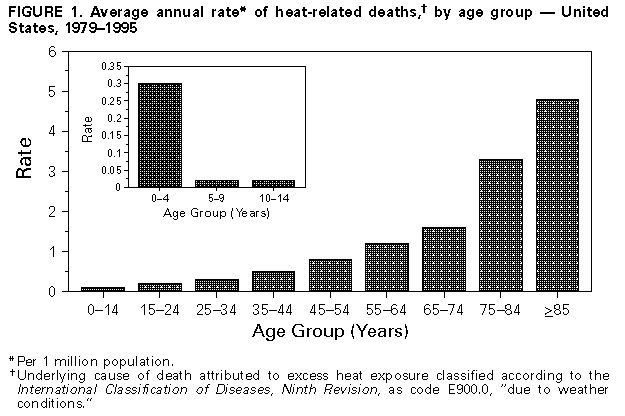 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}