 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Monitoring Environmental Disease -- United States, 1997One of the national health objectives for 2000 (HP2000) is to establish and monitor nonoccupational "sentinel" environmental diseases, including asthma, heatstroke, hypothermia, heavy metal poisoning, pesticide poisoning, carbon monoxide poisoning, acute chemical poisoning, and methemoglobinemia, in at least 35 states (baseline: 0 states in 1990) (objective 11.16) (1). To assess progress toward this objective, the Council of State and Territorial Epidemiologists (CSTE), the Association of Schools of Public Health, and CDC conducted a telephone survey of environmental epidemiologists in each of the 50 states, the District of Columbia, and Puerto Rico during June-August 1997. This report summarizes the results of that survey, which indicate that progress is being made toward the HP2000 objective. Approximately 2-3 weeks before the telephone survey was conducted, a questionnaire on environmental disease surveillance systems in each jurisdiction was sent to the epidemiologist responsible for environmental health to allow time for gathering of information. The questionnaire inquired about each jurisdiction's surveillance activities, sources of surveillance data, funding, and goals. Each jurisdiction was asked to describe its surveillance activities from among the following: data collection only; data collection and review; or data collection, review, and case investigation. No additional definitions were provided, and interpretation of the three classifications was left to the respondent. Responses were obtained from all 52 environmental epidemiologists. The telephone survey identified 174 environmental public health surveillance systems from 51 jurisdictions. The mean number of systems per jurisdiction was three; the median was two (range: zero to 12) (Figure_1). Of the 174, a total of 79 (45%) systems monitored lead exposure, with most systems monitoring childhood blood lead levels (BLLs) (51 {65%} of 79). The remaining 28 systems monitored nonoccupational adult lead exposures. The environmental diseases least frequently monitored were heatstroke and hypothermia (four systems each) (Table_1). One jurisdiction (Missouri) had surveillance systems for all 12 of the environmental public health conditions covered by the survey. One jurisdiction did not have any surveillance systems. Using the description for each disease monitoring system described in this report, 15 (9%) of the surveillance systems collected data only, 46 (27%) collected data and conducted reviews, and 110 (64%) collected data and conducted both reviews and case investigations. Asthma was the only condition for which no systems conducted case investigations. Sources of Data Data about environmental disease surveillance were collected from numerous sources. Of the 79 lead exposure surveillance systems, 76 (96%) provided information about primary source of data. Of these, 71 (93%) used laboratory data as the primary source of information. Laboratory reporting was mandatory in jurisdictions covered by 65 (86%) of 76 systems. Data about BLLs were gathered electronically by 35 (46%) systems. Five lead surveillance systems used electronic reporting exclusively. Of the remaining 95 nonlead environmental disease surveillance systems, three did not provide information about primary source of data. The sources of data for the other 92 systems included laboratories (37 {40%}), clinicians (19 {21%}), hospitals (14 {15%}), poison-control centers (seven {8%}), and other sources (15 {16%}). Laboratory reporting was mandatory in the jurisdictions covered by 27 (72%) of 37 systems gathering data from laboratories, and reporting by clinicians was mandatory in 15 (79%) of the 19 systems gathering data from clinicians. No nonlead surveillance systems received information electronically. Funding Thirty-six (71%) of 51 childhood lead monitoring systems and 14 (50%) of 28 adult lead monitoring systems were either entirely or largely dependent on federal funds for their operation. Twenty-one (23%) of 95 nonlead environmental disease monitoring systems received any federal funding. Reported by: P Zeitz, Rollins School of Public Health, Emory Univ; H Anderson, III, MD, B Hughes, PhD, Council of State and Territorial Epidemiologists, Atlanta, Georgia. Surveillance and Programs Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; and an EIS Officer, CDC. Editorial NoteEditorial Note: The findings in this report indicate that childhood lead poisoning was the only "sentinel environmental disease" for which HP2000 objective 11.16 has been achieved (1). Although not every system met the requirement to be identified as a surveillance system (ongoing collection, analysis, and use of health data), most of the childhood lead monitoring systems collected, reviewed, and took appropriate action based on the data. The findings in this report are subject to at least two limitations. First, jurisdiction-based surveillance systems can have different case definitions. For example, although CDC recommends using BLLs greater than or equal to 10 ug/dL to identify children with elevated BLLs, some jurisdictions used higher values. Jurisdiction-specific case definitions may be necessary because of limited resources and other considerations. CDC, in collaboration with other agencies and organizations, is developing definitions for several environmental diseases such as carbon monoxide poisoning and asthma. Using a standard case definition may allow data from numerous jurisdictions to be more easily summarized and compared. However, each jurisdiction will base its environmental health priorities on its own needs and available resources. Second, greater than 90% of the systems identified in the 1997 survey reviewed the data collected, and in most cases implemented activities based on the data. This survey did not collect information about the frequency or extent of data review or of follow-up activities. Usefulness of routinely collected environmental disease data depends on timely analysis of the data followed by dissemination of information to persons who "need to know," such as policy makers and program managers (2-7). Surveillance systems should be simple, sensitive, representative, and timely to be most effective in controlling and preventing disease (8). Surveillance systems at the local, state, and national levels are useful for assessing case investigations, implementing control activities, evaluating interventions, monitoring trends, and identifying risk factors. A comprehensive integrated public health surveillance system that combines local, state, and national surveillance activities can best achieve the primary goal of public health surveillance, namely a reduction in disease morbidity and mortality (3). Progress toward the HP2000 objective is evident from the results of this survey. Adequate resources and increased public awareness about the value of surveillance systems in preventing and controlling disease are necessary to fully achieve the objective (2). References
Figure_1 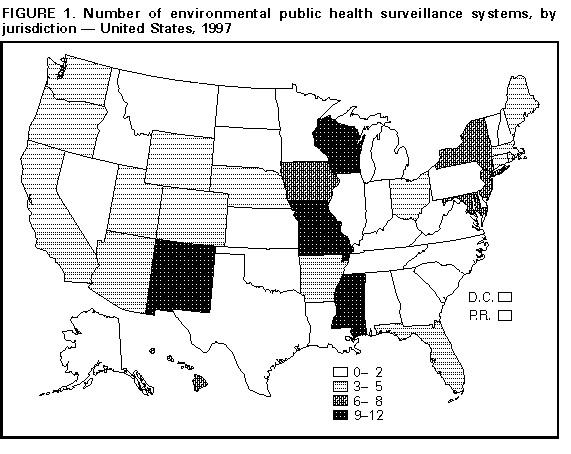 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Number of environmental public health surveillance systems, by type*
and classification of system -- United States,+ 1997
====================================================================================================
Classification
--------------------------------------------------
Data Data collection Data collection,
collection and review review, and case
Type of system only investigation Total
------------------------------------------------------------------------------------------------
Elevated blood lead levels 4 9 66 79
Children 1 2 48 51
Adults& 3 7 18 28
Pesticide poisoning 4 4 12 20
Mercury poisoning 0 6 8 15
Arsenic poisoning 0 4 6 11
Cadmium poisoning 0 4 6 11
Methemoglobinemia 2 2 5 9
Acute chemical poisoning@ 1 4 3 8
Carbon monoxide poisoning 3 2 2 7
Asthma 1 5 0 6
Heatstroke 0 3 1 4
Hypothermia 0 3 1 4
Total 15 46 110 174**
------------------------------------------------------------------------------------------------
* The 12 nonoccupational sentinel environmental conditions specified by the 2000 national
health objective 11.16 (1).
+ Includes District of Columbia and Puerto Rico.
& Excludes cases associated with occupational exposure.
@ Acids, ammonia, bases, chlorine, other inorganic substances, paints and dyes, volatile
organic compounds, and polychlorinated biphenyls.
** Includes three surveillance systems that included data collection and case investigation but
excluded routine review of cases.
====================================================================================================
Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}