 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
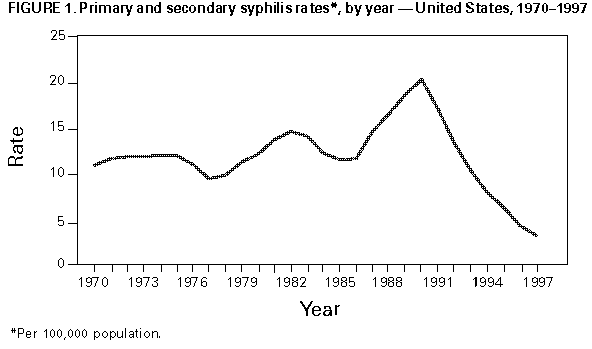
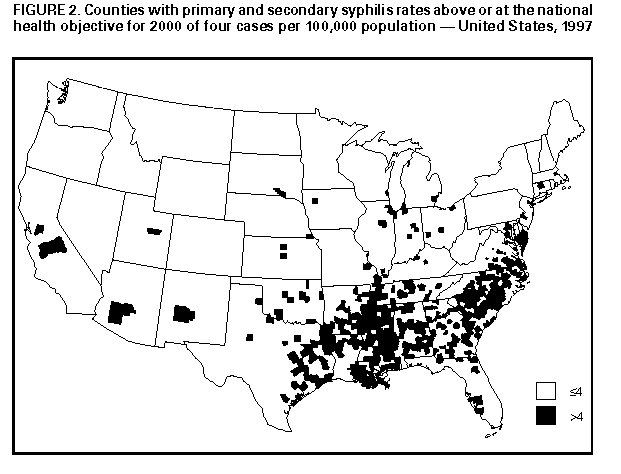
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Primary and Secondary Syphilis -- United States, 1997Syphilis is an acute and chronic sexually transmitted disease (STD) caused by infection with Treponema pallidum. The disease is characterized by skin and mucous membrane lesions in the acute phase (primary and secondary {P&S} syphilis) and lesions of the bone, viscera, and cardiovascular and neurologic systems in the chronic phase. Because syphilis enhances transmission of human immunodeficiency virus (HIV), prevention of syphilis is important for controlling HIV (1). During 1986-1990, an epidemic of syphilis occurred throughout the United States (2). Syphilis rates began to decline in 1991 and have declined each year since that time. To determine whether this decline is reflected in changes in the epidemiology of syphilis, CDC analyzed notifiable disease surveillance data for 1997. This report summarizes the findings of the analysis, which indicate that reported P&S syphilis cases declined 84% from 1990 to 1997, that syphilis remains substantially more common in non-Hispanic blacks than in other racial/ethnic groups, and that it continues to be concentrated in the Southern region of the United States. Summary data for syphilis cases reported to state health departments for 1997 were sent quarterly and annually to CDC. Data from states included the total number of syphilis cases by county, sex, stage of disease, racial/ethnic group, and 5-year age group. Data on reported cases of syphilis in the P&S stages were analyzed for this report because those cases best represent incident cases (i.e., newly acquired infections within the evaluated time period). P&S syphilis rates were calculated per 100,000 persons using population denominators from the Bureau of Census (2). In 1997, the incidence of P&S syphilis in the United States was 3.2 per 100,000 population (Figure_1). Rates of P&S syphilis were higher in the South (6.6 per 100,000 population) than in the Midwest (2.0), Northeast (1.1), and West (1.0). * The South is the only region that has not achieved the revised national health objective for 2000 (HP2000) of four cases per 100,000 population (objective 19.3) (2). In 1997, a total of 41 (82%) states had P&S syphilis rates below the HP2000 objective, and 21 states (42%) reported 10 or fewer cases of P&S syphilis (Table_1). Montana, New Hampshire, North Dakota, Vermont, and Wyoming reported zero cases of P&S syphilis. No cases of P&S syphilis were reported in 1997 from 2324 (75%) of 3115 counties. Rates of P&S syphilis were below the HP2000 objective in 2698 (86%) counties. A total of 31 (1.0%) counties accounted for 50% of P&S syphilis cases, and 186 (6%) counties accounted for 85% of all reported P&S syphilis cases (Figure_2). P&S syphilis rates for blacks remained substantially higher than those for non-Hispanic whites and Hispanics. In 1997, the P&S syphilis rate for blacks was 22.0 per 100,000, compared with 1.6 for Hispanics and 0.5 for non-Hispanic whites. The overall male-to-female P&S syphilis rate ratio was 1.2; this rate ratio was higher for Hispanics (2.1) than for blacks (1.3) and non-Hispanic whites (1.2). P&S syphilis rates were highest for Hispanic women aged 15-19 years (2.7), for black women aged 20-24 years (47.9), and for non-Hispanic white women aged 25-39 years (1.2). P&S syphilis rates were highest for Hispanic men aged 25-29 years (5.5) and for black and non-Hispanic white men aged 35-39 years (50.6 and 1.2, respectively). From 1990 to 1997, P&S syphilis rates declined 84% in the United States, in all regions (95% in the Northeast, 91% in the West, 80% in the South, and 73% in the Midwest), and in all but two states (Indiana and Kentucky). Rates in Indiana and Kentucky peaked in 1993 and have declined steadily since that time. Rates of P&S syphilis were below the revised HP2000 objective in 86% of all counties in 1997, compared with 69% in 1990. P&S syphilis rates have declined for all racial/ethnic groups; the largest decline occurred among Hispanics (90%) followed by blacks (85%) and non-Hispanic whites (81%). The P&S syphilis male-to-female rate ratio has remained stable for all races. Reported by: Div of Sexually Transmitted Diseases Prevention, National Center for HIV, STD, and TB Prevention, CDC. Editorial NoteEditorial Note: The findings in this report document substantial progress in the control and prevention of infectious syphilis in the United States. P&S syphilis is at its lowest level since reporting began in 1941. Although syphilis remains an endemic disease in parts of the South, rates in this region have declined 80% since 1990. The South has had the highest syphilis rates since the 1940s, in part because of limited access to health care in many parts of the South. Despite substantial declines in P&S syphilis in all racial/ethnic groups, syphilis continues to disproportionately affect blacks. Reporting of syphilis has presumably been biased toward over-reporting of infections in persons of minority races/ethnicities who attend public STD clinics; the degree to which this bias influences disease rates across racial/ethnic groups is unknown. Reasons for these reported racial disparities require further investigation. At least four factors may have contributed to the recent decline in syphilis. First, after recognition of the epidemic in the mid-1980s, increased state and federal resources were invested in syphilis control programs (3). These resources were used for both traditional (e.g., partner notification and clinical services) and nontraditional (e.g., community-based screening and outreach and risk-reduction counseling) activities (3). Second, since the mid-1980s, a variety of HIV prevention activities have been implemented throughout the United States. Although these activities probably contributed to declines in all STDs, it is unknown how these activities contributed to the prevention of specific bacterial STDs. Third, a decline in crack cocaine use (4) may have resulted in a decline in the incidence of syphilis. Use of crack cocaine and exchange of sex for drugs were major contributors to the recent syphilis epidemic (5). Finally, the presence of acquired immunity in the population at risk following the epidemic may have contributed to the decline (6,7). A concerted effort while rates are low and disease is focal could contribute to the possible elimination of domestic transmission of syphilis in the United States (8). In 1996, the Council of State and Territorial Epidemiologists proposed that syphilis surveillance systems be evaluated and strengthened, that treatment and prevention efforts be enhanced in areas of substantial ongoing transmission, that a national workgroup be convened to evaluate the possibility of elimination of domestic syphilis transmission, and that ongoing support for syphilis control be maintained or enhanced until domestic syphilis is eliminated. A recent Institute of Medicine report on STDs in the United States suggests that STD surveillance systems use new information technology, be accurate and timely enough to identify national and local trends in STD incidence, and provide the data necessary to direct local activities (9). CDC is working toward improving syphilis surveillance on a national level by encouraging state and local health departments to discontinue aggregate syphilis reporting and to collect, analyze, take action on, and report line-listed case reports of syphilis electronically to CDC. These line-listed data will provide an opportunity to analyze case reports at the county level by a variety of demographic characteristics and other potential risk factors for STD. Syphilis is increasingly manifested as an epidemic rather than an endemic disease in the United States; focal outbreaks are still occurring (5). Optimal combinations of several different prevention and control strategies may be useful for areas with different levels of morbidity (i.e., to prevent importation into those areas without disease and to intensify detection and control in those areas with substantial morbidity). Several state and local health departments have developed enhanced syphilis control and elimination plans (e.g., California, Florida, Massachusetts, and San Diego County). Components of such a plan could include an evaluation and enhancement of the surveillance system, a review of the epidemiology of syphilis in the local area and development of targeted interventions if applicable, and enhancement of screening for syphilis in high-risk populations (e.g., correctional and drug-treatment facilities and emergency departments). References
+-------------------------------------------------------------------
-------+
|
|
| Erratum: Vol 47, No. 24
|
| ***********************
|
|
|
| SOURCE:47(27);574 DATE:Jul 17 1998
|
|
|
| In the article "Primary and Secondary Syphilis -- United
States, |
| 1997," on page 493 the last sentence in the first paragraph
should read |
| "This report summarizes the findings of the analysis, which
indicate |
| that 8551 cases of primary and secondary (P&S) syphilis were
reported |
| in 1997, an 83% decline in cases from the peak of the epidemic
in 1990, |
| and that syphilis remains substantially more common in
non-Hispanic |
| blacks than in other racial/ethnic groups and continues to be be
|
| concentrated in the Southern region of the United States."
|
|
|
+-------------------------------------------------------------------
-------+ TABLE 1. Reported primary and secondary syphillis rates *, by state and sex -- United States, 1997 ========================================== State Male Female Total ------------------------------------------ Alabama 11.1 8.2 9.6 Alaska 0.3 0 0.2 Arizona 4.3 1.7 3.0 Arkansas 5.8 7.9 6.9 California 1.7 0.7 1.2 Colorado 0.5 0.3 0.4 Connecticut 2.3 1.5 1.9 Delaware 3.4 2.7 3.0 Florida 2.4 1.8 2.1 Georgia 9.0 5.1 7.0 Hawaii 0.2 0 0.1 Idaho 0.2 0 0.1 Illinois 4.2 3.2 3.7 Indiana 2.4 2.7 2.6 Iowa 0.2 0.3 0.2 Kansas 1.4 0.8 1.1 Kentucky 3.7 3.3 3.5 Louisiana 8.4 8.3 8.4 Maine 0.2 0.2 0.2 Maryland 19.8 15.4 17.6 Massachusetts 1.5 1.0 1.3 Michigan 1.8 1.4 1.6 Minnesota 0.5 0.2 0.3 Mississippi 14.5 14.2 14.4 Missouri 2.1 2.2 2.1 Montana 0 0 0 Nebraska 0.4 0.2 0.3 Nevada 0.5 0.8 0.6 New Hampshire 0 0 0 New Jersey 2.4 1.4 1.9 New Mexico 0.5 0.6 0.5 New York 0.9 0.6 0.8 North Carolina 10.3 9.4 9.8 North Dakota 0 0 0 Ohio 2.2 1.8 2.0 Oklahoma 4.0 3.1 3.5 Oregon 0.5 0.1 0.3 Pennsylvania 1.2 0.8 1.0 Rhode Island 0.2 0.2 0.2 South Carolina 11.5 9.0 10.2 South Dakota 0.3 0 0.1 Tennessee 14.7 13.5 14.0 Texas 3.8 3.3 3.5 Utah 0.3 0.2 0.2 Vermont 0 0 0 Virginia 3.8 3.3 3.5 Washington 0.3 0.3 0.3 West Virginia 0.1 0 0.1 Wisconsin 1.6 1.9 1.7 Wyoming 0 0 0 Total 3.6 2.9 3.2 ------------------------------------------ * Per 100,000 population. ========================================== Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}