 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Leptospirosis and Unexplained Acute Febrile Illness Among Athletes Participating in Triathlons -- Illinois and Wisconsin, 1998Since July 14, 1998, the Illinois Department of Health, the Wisconsin Department of Health, the U.S. Department of Agriculture (USDA), and CDC, in collaboration with other state and local health departments, have been investigating an outbreak of acute febrile illness among athletes from 44 states and seven countries who participated in triathlons * in Springfield, Illinois, on June 21, 1998, and in Madison, Wisconsin, on July 5, 1998 (1). Initial testing at CDC of specimens from four athletes identified leptospirosis as the illness in all four (1). This report updates the ongoing investigation of this outbreak through August 13, which indicates that Leptospira was the etiologic agent for illness in athletes and in persons with occupational or recreational exposure to Lake Springfield, where the event was held in Illinois. To identify cases of febrile illness, a standardized telephone survey was conducted of athletes who participated in the event in Illinois, the event in Wisconsin, or both events. Including late registrants and excluding preregistrants who did not participate in either event, respondents included 733 (95%) of 775 athletes who participated only in the Illinois event, 370 (67%) of 553 athletes who participated only in the Wisconsin event, and 91 (95%) of 96 athletes who participated in both events. A suspected case of leptospirosis was defined as onset of fever during June 21-August 13 in a triathlon participant that was associated with at least two of the following symptoms or signs: chills, headache, myalgia, diarrhea, eye pain, or red eyes (1). Of the 1194 athletes surveyed, 110 (9%) who participated in one or both events described an illness meeting the case definition; no cases occurred after July 24. The median age of suspected case-patients was 35 years (range: 15-80 years); 76% were male. Ill athletes were similar in age and sex to athletes who were not ill. Of the 110, a total of 73 (66%) sought medical care; 23 (32%) of those were hospitalized. Attack rates among respondents varied by triathlon site: 84 (11%) Illinois-only participants; 20 (5%) Wisconsin-only participants; and six (7%) athletes participating in both events. Compared with Wisconsin-only participants, Illinois-only participants were more likely to have had an illness meeting the case definition (relative risk {RR}=2.0; 95% confidence interval {CI}=1.3-4.0). Illinois-only case-patients also were more likely to have had chills, myalgias, or headache than Wisconsin-only case-patients (pless than 0.05); however, diarrhea was less common among Illinois-only case-patients. In addition, illness in Illinois-only case-patients had longer incubation periods (days from event to onset of fever: 14 days {Illinois-only} versus 7 days {Wisconsin-only}; pless than 0.01). Illinois-only case-patients were more likely to seek medical care than Wisconsin-only case-patients (RR=1.8; 95% CI=1.2-2.8). All 23 hospitalized athletes participated in the Illinois triathlon; none of the athletes participating only in the Wisconsin event were hospitalized. Laboratory evidence for leptospirosis was defined as 1) a positive result for Leptospira on screening IgM enzyme-linked immunosorbent assay (ELISA) with confirmatory testing by a single microagglutination test (MAT) titer of greater than or equal to 400, or a four-fold or greater rise in MAT titer between acute-phase and convalescent serum specimens (2); 2) a positive tissue immunohistochemical (IHC) stain using rabbit polyclonal reference antiserum reactive with 16 different leptospiral strains (3); or 3) a positive culture. Acute-phase serum specimens have been tested for 374 of 871 athletes who participated in the Illinois triathlon; 70 of these specimens were obtained from the 90 athletes whose illness met the case definition (Figure_1). Acute-phase serum specimens from 30 (43%) of these 70 case-patients and serum specimens from three (1%) of 304 athletes who had illness not meeting the case definition tested positive by ELISA. Of the 30 case-patients with a positive ELISA, 24 tested positive by confirmatory MAT with highest titers to pathogenic Leptospira serovars grippotyphosa, bratislava, and djasiman. In comparison, acute-phase serum specimens have been tested for 70 of 553 athletes who participated in only the Wisconsin triathlon, including 10 specimens from the 20 athletes whose illness met the case definition; none tested positive. Because serologic response can be delayed, convalescent specimens are required to interpret accurately serologic test results; paired, 2-week convalescent serum specimens are being obtained for all athletes whose acute-phase serum specimens have been tested. No positive cultures for Leptospira have been identified in either group of athletes. On July 24, the Springfield and the Illinois departments of health issued a precautionary advisory not to swim, water ski, or use personal watercraft at Lake Springfield. To identify Springfield residents with only occupational or recreational exposure to Lake Springfield, the Springfield Department of Health initiated active and passive surveillance using the same case definition without specified time constraints. A total of 228 community case-patients in Springfield have been identified; 146 (64%) have had acute-phase serum specimens tested at CDC by ELISA. Specimens from five of these persons were positive by ELISA. Of these five, confirmatory testing by MAT has been performed for four; leptospirosis was confirmed in three case-patients, and confirmation for the fourth case-patient will require further testing of convalescent serum. Two hospitalized community residents who are suspected case-patients (serum specimens have yet to be tested) and who were treated with intravenous (IV) penicillin developed a Jarisch-Herxheimer reaction (a transient immunologic reaction following antibiotic treatment) (4) requiring hemodynamic support. CDC, in collaboration with USDA and state and local health departments, is continuing epidemiologic, laboratory, and environmental investigations of these outbreaks. The objectives are to 1) identify additional cases of leptospirosis among athletes and among occupational and recreational users of Lake Springfield, 2) determine the etiology of illness and identify the source and mode of transmission among athletes who participated in only the Wisconsin triathlon, and 3) develop prevention and control measures for both outbreaks. Reported by: Wisconsin Outbreak Investigation Team, Wisconsin Div of Health. Illinois Outbreak Investigation Team, Springfield Dept of Health and Illinois Dept of Public Health. Council of State and Territorial Epidemiologists, Atlanta, Georgia. Zoonotic Diseases Research Unit, Agriculture Research Svc, US Dept of Agriculture. Meningitis and Special Pathogens Br, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; and EIS officers, CDC. Editorial NoteEditorial Note: Leptospirosis is an acute febrile illness with a typical incubation period ranging from a few days to 4 weeks that usually begins abruptly with fever, chills, rigors, myalgia, and headache, and may include conjunctivitis, abdominal pain, vomiting, diarrhea, skin rashes, and meningeal symptoms (5). The acute septicemic phase can be followed by a secondary phase of severe disease characterized by aseptic meningitis, jaundice, renal failure, hemorrhage, or hemodynamic collapse. Mild infections can be treated with oral doxycycline; patients requiring hospitalization should be treated with IV penicillin (1,5). Epidemiologic, serologic, and IHC staining evidence suggest that Leptospira was the etiologic agent causing disease among the athletes who participated in the Illinois triathlon. Similar illness and serologic confirmation among persons with occupational and recreational exposure to the same lake where the event was held support this theory. Athletes who participated in only the Wisconsin triathlon have demonstrated a different spectrum of symptoms and signs, have had a less severe illness, and have lacked serologic evidence for leptospirosis. However, additional serologic testing for leptospirosis among these athletes and additional testing for viral agents are needed. Establishing an epidemiologic link between species of Leptospira obtained through environmental sampling (e.g., testing water, mud, and wild and domestic animals) and pathogenic serovars of Leptospira causing illness in humans in the same environments can be particularly difficult. Pathogenic Leptospira infect a variety of domestic and wild animals that subsequently excrete the organism in their urine. In temperate climates, both pathogenic and saprophytic Leptospira species can be found in fresh water, damp soil, vegetation, and mud, particularly during summer months (6). Therefore, no natural body of water can be expected to be free of Leptospira. Pathogenic and saprophytic Leptospira species obtained from environmental samples can be distinguished through a variety of tests, including molecular diagnostic testing (6-8); however, these techniques are difficult and time-consuming. The identification by culture or MAT of specific serovars causing leptospirosis in humans may facilitate identification of potential animal reservoirs (domestic and/or wild) of the environmental contamination. Although leptospirosis has not been described among competitive athletes (9), recreational exposure to natural water sources is a common route of transmission (7). In the absence of a defined source of prior or continued contamination of Lake Springfield with pathogenic Leptospira, enhanced passive and active surveillance for symptoms and signs of illness of leptospirosis will be necessary to monitor the safety of recreational use of Lake Springfield. Additional information regarding this outbreak is available from CDC, telephone (888) 688-2732 ({888} OUTBREAK); on the World-Wide Web site, http://www.cdc.gov/ncidod/dbmd/lepto.htm; or through state and local health departments. References
A triathlon is a race consisting of swimming, biking, and running competitions. Figure_1 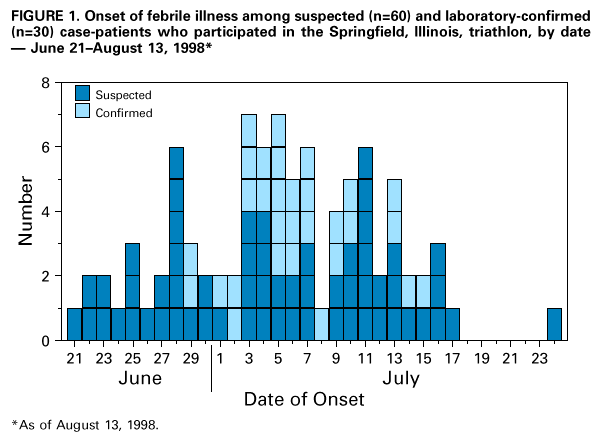 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/05/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}