 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Measles Control and Regional Elimination, 1990-1997In 1989, the World Health Assembly resolved to reduce measles morbidity and mortality by 90% and 95%, respectively, by 1995, compared with disease burden during the prevaccine era (1). In 1990, the World Summit for Children adopted a goal of vaccinating 90% of children against measles by 2000. Regional measles-elimination goals have been established in the American Region (AMR) by 2000, the European Region (EUR) by 2007, and the Eastern Mediterranean Region (EMR) by 2010. This report updates progress toward global measles control and regional elimination (2), and presents measles vaccination coverage and incidence for 1997* and WHO estimates of global measles morbidity and mortality in 1997 compared with the prevaccine era**. Reported Measles Morbidity and Routine Vaccination Coverage In 1997, 702,298 cases were reported to WHO, a 48% decline compared with 1990 (3 ). Among the six WHO regions***, the African Region (AFR) reported the highest measles incidence (47.5 per 100,000), and AMR reported the lowest (6.5 per 100,000). However, the 51,915 cases of measles reported from AMR in 1997 represent a 25-fold increase over the record low 2109 cases in 1996 (2,3). The increase resulted from a measles outbreak of greater than 42,000 confirmed cases in S o Paulo State, Brazil, that spread to other states in Brazil and to other countries in the region (4,5). Vaccination coverage data were based on reports provided by member states to WHO and adjusted for the target population (annual number of infants surviving their first year of life) (3). Since 1990, global routine vaccination coverage among children aged 1 year with one dose of measles vaccine has remained relatively stable at approximately 80% (Figure_1). In 1997, reported global coverage was 82%; vaccination coverage was 93% in AMR and the Western Pacific Region (WPR). The lowest vaccination coverage (57%) was reported from AFR, where only two (4%) of 48 countries reported vaccination coverage of greater than or equal to 90%, and 10 (21%) countries reported routine coverage of less than 50%. Approximately 346 million children, 57% of the world's children aged less than 5 years, reside in the countries that either reported routine measles vaccination coverage of less than 90% or did not provide a report in 1997. More than two thirds of these children reside in Africa and South East Asia (Table_1). Estimated Morbidity and Mortality Because measles deaths are not reported routinely to WHO, measles is not a notifiable disease in some countries, and underreporting of measles occurs in all regions, each year WHO estimates actual measles morbidity and mortality. These estimates are based on the annual number of surviving infants, reported vaccination coverage data (routine and mass campaigns), and average vaccine effectiveness and case-fatality rates based on published literature. For 1997, WHO estimated that approximately 31 million measles cases and 960,000 measles-related deaths occurred worldwide (Table_2). By the end of 1997, global measles morbidity and mortality had decreased 74% and 85%, respectively, compared with the annual morbidity and mortality during the prevaccine era. AMR and WPR reached the 1995 morbidity and mortality reduction goals of the World Health Assembly; EUR reached the mortality reduction goal. When grouped by economic development status, 99% of the estimated measles deaths in 1997 occurred in the least developed and developing countries and less than 1% in developed countries or countries in economic transition. Supplementary Vaccination Campaigns In 1994, the ministries of health of AMR resolved to eliminate indigenous measles transmission from the Western Hemisphere by 2000 using a three-vaccination component strategy (i.e., "catch-up," "keep-up," and "follow-up"****) and enhanced surveillance with laboratory investigation of suspected cases (5,6). By the end of 1996, all countries in AMR, except the United States, French Guiana, and several Caribbean islands, had catch-up campaigns. Most countries of AMR also have completed follow-up campaigns (Figure_2). Outside AMR, catch-up campaigns have been used increasingly to supplement routine vaccination in countries targeting outbreak prevention or measles elimination (Figure_2). Countries in EUR (i.e., the United Kingdom), WPR (i.e., Mongolia, New Zealand, and the Pacific Island nations), AFR (i.e., Southern African countries), EMR (i.e., Bahrain, Jordan, Kuwait, and Oman), and the South East Asian Region (SEAR) (i.e., Bhutan and Maldives) have completed catch-up campaigns. In 1997, 32.8 million children were vaccinated as part of catch-up or follow-up campaigns. As of November 1998, catch-up campaigns were ongoing in Australia, the Philippines, Romania, Syran Arab Republic, and Tunisia. Supplementary measles vaccination campaigns in high-risk areas, such as densely populated cities in developing countries, have been implemented to reduce measles mortality and accelerate measles control. In 1997, vaccination campaigns were implemented in high-risk areas for measles in 10 countries (five in AFR, four in SEAR, and one in WPR). These campaigns reached approximately 5.8 million children. Reported by: Expanded Program on Immunization, Dept of Vaccines and Other Biologics, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Measles Activity, Epidemiology and Surveillance Div, and Vaccine Preventable Disease Eradication Div, National Immunization Program; and an EIS Officer, CDC. Editorial NoteEditorial Note: Despite the widespread availability of safe and effective measles vaccines since 1963, measles still accounts for approximately 1 million deaths annually (7 ). Measles was the eighth leading cause of death worldwide in 1990, representing 2.7% of disability-adjusted life years (7). Measles remains highly endemic in several countries in Europe, Asia, and Africa, irrespective of level of economic development. However, measles-related deaths occur almost exclusively in developing countries. Routine measles vaccination coverage at the global level reached 80% in 1990, and has shown minimal progress from 1990 through 1997. Routine global coverage conceals large differences in coverage levels attained by the six WHO regions and among countries within regions. AMR and WPR achieved the World Summit for Children coverage goal; however, both regions have countries with coverage of less than 90%. AMR, EMR, and EUR have begun regional measles elimination and continue to make progress toward achieving the goal. In 1996, implementation of measles-elimination strategies by the Pan American Health Organization (PAHO) (5,6) resulted in the lowest measles incidence ever reported by a WHO region and in elimination of measles-related deaths in AMR. In 1998, EMR held two workshops to develop plans for accelerated measles control or elimination, and Persian Gulf countries (i.e., Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and United Arab Emirates) established a target of measles elimination by 2000. In EUR, the goal of eliminating measles by 2007 was endorsed by the 48th Regional Committee in September 1998. In addition, six AFR countries (Botswana, Malawi, Namibia, South Africa, Swaziland, and Zimbabwe) adopted national measles-elimination goals. Effective measles surveillance is critical for monitoring the impact of vaccination activities and adapting policies and strategies. Further strengthening of measles surveillance systems is required both in developing and developed countries. Measles surveillance, which combines epidemiologic data and virologic surveillance, is necessary when incidence of disease decreases to low levels following intensive outbreak-prevention and/or measles-elimination measures (4). To facilitate virologic surveillance, a standardized nomenclature for describing the genetic characteristics and relations among eight groups of wild-type measles viruses has been proposed (8 ). Progress toward achieving global measles reduction and vaccination coverage goals by 2000 primarily depends on future performance of vaccination programs. To accelerate measles control and achieve regional elimination, three vaccination-related priority areas should be addressed. First, strengthening of infrastructures necessary to improve global routine vaccination coverage among infants and young children is needed. Second, supplementary mass vaccination campaigns designed to reach children not covered by routine services are needed in low-income countries to reduce measles-related deaths (4). Any supplemental vaccination campaign in high-risk areas should reach all children in the target age range regardless of measles vaccination status or history of previous measles disease (4). Third, in countries with measles-elimination goals, the highest coverage possible (greater than 90%) in the catch-up and subsequent follow-up campaigns is needed to achieve and maintain interruption of indigenous measles virus transmission. The phased implementation of accelerated measles control/elimination activities must facilitate and not jeopardize the current global poliomyelitis eradication initiative that is now at an advanced stage. Measles-control activities in countries where polio is endemic or countries with focal poliovirus transmission should target morbidity and mortality reduction (9). Measles elimination in the Western Hemisphere by 2000 is possible if vaccination and surveillance activities are rapidly intensified in the remaining countries with continuing transmission. In July 1996, WHO, PAHO, and CDC cosponsored a meeting where participants concluded that global measles eradication was technically feasible with available vaccines (10). Initiation of a global effort to eradicate measles early in the 21st century will require completion of global polio eradication and continued progress toward interruption of indigenous transmission of measles in the Western Hemisphere. References
* Reported to the World Health Organization (WHO) as of July 20, 1998. ** Number of measles cases during the prevaccine era was estimated by WHO on a country-by-country basis, and assumed equivalent to 95% of the surviving infants in 1980 for most developing countries, or in 1975 for developed countries. Surviving infants were defined as all live-born infants during a 1-year period minus the number of deaths during the first year of life. *** African, American, Eastern Mediterranean, European, South East Asian, and Western Pacific regions. **** Catch-up is defined as a one-time, nationwide vaccination campaign targeting usually all children aged 9 months-14 years, regardless of history of measles disease or vaccination status; keep-up is defined as routine services aimed at vaccinating 90% of each successive birth cohort; and follow-up is defined as subsequent nationwide vaccination campaigns conducted every 2-5 years targeting usually all children born after the catch-up campaign. Figure_1 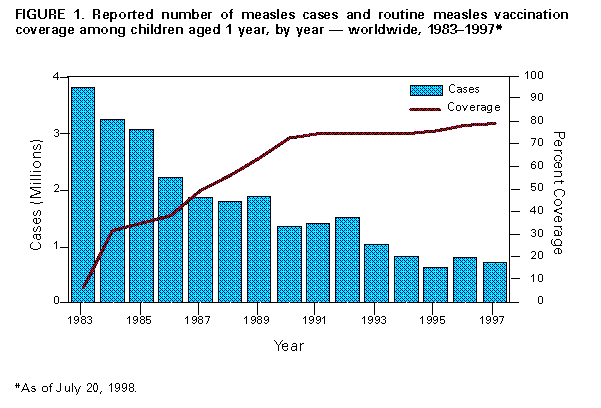 Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Reported measles cases, reported routine vaccination coverage among children aged 1 year, and progress toward achievement of vaccination coverage goals, by World Health Organization (WHO)
region -- worldwide, 1990 and 1997 *
==================================================================================================================================================================================================================
1997
-------------------------------------------------------------------
No. children @ aged <5 years
Reported cases + Reported coverage & residing in countries with
------------------------------------------- ------------------------------------- No. countries with coverage coverage
% Change from 1990 % Change from 1990 ------------------------------ ----------------------------------
Region 1990 1997 to 1997 1990 1997 to 1997 1997 Incidence <90% or unknown >=90% <90% or unknown >=90%
------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
African 481,294 290,942 -40% 53% 57% 4% 47.5 46 2 107.2 0.2
American 246,607 51,915 -80% 77% 93% 16% 6.5 20 27 12.5 63.2
Eastern Mediterranean 59,502 33,342 -44% 77% 83% 6% 7.5 7 16 32.9 39.1
European 188,306 103,129 -45% 79% 87% 8% 11.9 25 26 38.3 16.0
Southeast Asian 225,144 114,331 -49% 85% 85% 0 7.8 6 4 128.1 37.2
Western Pacific 156,139 108,639 -30% 93% 93% 0 6.6 24 12 27.4 110.2
Total 1,356,992 702,298 -48% 80% 82% 2% 12.0 128 87 346.4 265.9
------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
* Reported to WHO as of July 20, 1998.
+ Reported cases from 197 and 198 countries in 1990 and 1997, respectively.
& Reports received from countries representing 94% and 88% of global population in 1990 and 1997, respectively.
@ In millions.
==================================================================================================================================================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Estimated annual number of measles cases and deaths and progress toward achieving measles morbidity and mortality reduction goals in 1997
compared with the prevaccine era, by World Health Organization region
==================================================================================================================================================================
Estimated annual cases in 1997 Estimated % Reduction in Estimated annual deaths 1997 Estimated % Reduction in
Region prevaccine era cases cases* in prevaccine era deaths deaths*
------------------------------------------------------------------------------------------------------------------------------------------------------------------
African 14,477,000 11,439,541 48% 1,309,000 549,125 73%
American 13,277,000 53,661 99% 695,000 61+ 99%
Eastern Mediterranean 10,536,000 4,444,713 70% 767,000 111,114 90%
European 12,085,000 1,923,217 81% 151,000 6,509 95%
South East Asian 30,597,000 9,586,577 70% 2,142,000 268,482 88%
Western Pacific 25,485,000 3,531,880 90%& 720,000 25,188 97%
Total 106,457,000 30,979,589 74% 5,784,000 960,479 85%
------------------------------------------------------------------------------------------------------------------------------------------------------------------
* Adjusted for population growth.
+ Reported number of measles cases and deaths as of December 8, 1998. The Pan American Health Organization estimates that the completeness of reporting
for measles cases and deaths is nearly 100%.
& Based on Western Pacific regional office estimate.
==================================================================================================================================================================
Return to top. Figure_2 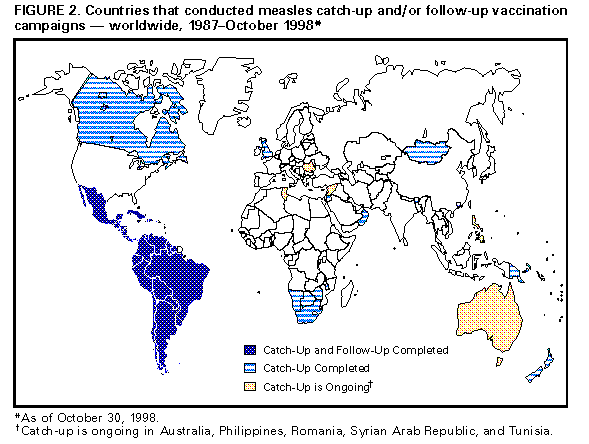 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 12/14/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}