 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Epidemiology of Measles -- United States, 1998During 1998, a provisional total of 100 confirmed measles cases was reported to CDC by state and local health departments, representing a record low number of cases and 28% fewer than the 138 cases reported in 1997 (1). This report describes the epidemiology of measles during 1998, which suggests that measles is no longer an indigenous disease in the United States. Case Classification Measles cases among persons who were infected outside the United States are classified as internationally imported cases. Cases among persons who were infected in the United States are classified as indigenous measles cases. Indigenous cases are subclassified into three groups: cases epidemiologically (epi)-linked to importation (a chain of transmission caused by an internationally imported case); imported virus cases (a chain of transmission from which an imported measles virus strain was isolated but a link to an internationally imported case was not identified) (2); and not importation-associated cases (no epidemiologic or virologic association to importation was detected). Internationally imported cases, cases epi-linked to importation, and imported virus cases are all considered importation-associated cases. Of the 100 cases reported, 26 were internationally imported, and 74 were indigenous. Of the 74 indigenous cases, 45 were importation-associated, and 29 were not importation-associated. The proportion of cases not associated with importation has declined from 85% in 1995, 72% in 1996, 41% in 1997, to 29% in 1998. The 45 importation-associated indigenous cases included 13 epi-linked cases and 32 imported virus cases. All 32 imported virus cases occurred in an outbreak in Alaska, which started 4 weeks after an imported case of measles was diagnosed in a visitor from Japan. Measles virus isolated from cases in this outbreak was nearly identical to virus circulating in Japan, although no virus was cultured from the imported case and no epidemiologic link between the imported case and the outbreak was detected (3). In addition to the strain isolated from the Alaska outbreak, viral genomic sequencing of specimens from epi-linked cases allowed genotype classification of measles virus strains from six chains of transmission epidemiologically linked to internationally imported cases. Virus strains isolated from cases in New York, Vermont, California, Massachusetts, and Washington matched viral genotypes from Germany, Cyprus, Japan, China, and Croatia, respectively. Measles virus was isolated from the Indiana outbreak but genotype information was unavailable from Zimbabwe, the source country of the imported case. Internationally Imported Measles Cases The 26 internationally imported cases reported in 1998 represent the lowest number of imported cases since the recording of importation status began in 1983. Imported cases from the Americas remained at very low levels, and imported cases from Europe and Asia declined compared with the previous 4 years (Figure 1). India, Japan, Kenya, Pakistan, and Saudi Arabia each were the source of two imported cases. One importation was reported from each of the other countries. Of 26 imported cases, 14 occurred among international visitors and 12 occurred among U.S. residents exposed to measles while traveling abroad. Geographic Distribution During 1998, 28 states and the District of Columbia reported no confirmed measles cases, compared with 21 states in 1997. Eight states accounted for 82% of cases: Alaska (33 cases), Arizona (11), Michigan (10), California (nine), New Jersey (eight), New York (four), Pennsylvania (four), and Indiana (three). In the remaining 14 states, two or fewer cases were reported. Eight states reported indigenous measles cases not associated with importation. Temporal Patterns of Transmission The median number of cases per week was one (range: 0-11). During 35 weeks, all reported measles cases were importation-associated, including 21 consecutive weeks (weeks 25-45) (Figure 2). Half of the indigenous cases that were not importation-associated occurred in two outbreaks: in New Jersey (weeks 13-16) and in Michigan (weeks 20-23). Age and Vaccination Status The age distribution and vaccination status of U.S. residents with measles differed from those of international visitors. Most U.S. residents with measles had been vaccinated with one or more doses of measles vaccine (53%), and 86% of international visitors with measles were unvaccinated. Outbreaks Six measles outbreaks* were reported in 1998, the fewest ever reported to CDC. Outbreaks occurred in Alaska (33 cases), Arizona (11), Michigan (nine), New Jersey (six), Indiana (three), and Pennsylvania (three). The 65 measles cases reported from these outbreaks represented 65% of all cases reported during 1998. The ages of persons with outbreak-associated cases ranged from 5 months to 44 years (median: 15 years). The largest measles outbreak reported since 1996 occurred in a high school in Anchorage, Alaska; 30 of the 33 cases had received one dose of measles vaccine. A 4-year-old unvaccinated Japanese child visiting Anchorage had measles diagnosed 4 weeks before the other cases in the outbreak. No epi-link was reported between this case and subsequent cases. However, the genotype of viral RNA collected from outbreak cases was nearly identical to virus circulating in Japan. The interval from the onset of rash in the imported case to the end of the outbreak was 15 weeks (August 10 to November 19, the longest interval of transmission in 1998). As a result of the outbreak, the Alaskan Health Department now requires two doses of measles vaccine for all students in grades K-12 (3).Three outbreaks (Arizona, Indiana, and Pennsylvania) were epi-linked to an imported measles case, and two outbreaks (Michigan and New Jersey) were not importation-associated. Reported by: State and local health depts. Measles Virus Section, Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Measles Elimination Activity, Child Vaccine Preventable Diseases Br, Epidemiology and Surveillance Div, National Immunization Program; and an EIS Officer, CDC. Editorial Note:Analysis of epidemiologic data for 1998 suggests measles is no longer an indigenous disease in the United States. Most cases reported in 1998 were associated with importation, including the short chains of indigenous transmission of measles that occurred following international importation of measles. Cases not associated with importation were insufficient to represent a continuous indigenous chain of measles transmission and probably were misclassifications (not measles), associated with undetected imported measles cases, or linked to known imported cases through chains of transmission not detected by the surveillance system. Misclassifications resulting from false-positive laboratory tests are an expected result of intensive investigation for a rare disease using a laboratory test that is not 100% specific. Some cases may spread from undetected imported cases of measles. Detecting imported cases is difficult. International visitors with measles may leave the country before the rash appears or before they seek medical care. Even when the imported case is detected, it is difficult to detect every case in the chain of transmission, as was seen in the outbreak in Alaska. This highlights the need to obtain viral specimens from every chain of transmission to supplement epidemiologic information. The largest outbreak in 1998 occurred in a high school without a second dose measles vaccine requirement (3). As of the 1998-99 school year, 55% of U.S. students were required by their states to have two doses of measles vaccine (CDC, unpublished data, 1998). Vaccination of all students with two doses of measles vaccine by 2001, as recommended by the American Academy of Pediatrics (4) and CDC's Advisory Committee on Immunization Practices (5), will reduce future school outbreaks. Completion of this strategy should further decrease the risk for indigenous transmission of measles following importation of the measles virus. The United States appears to have eliminated measles as an indigenous disease. High measles vaccination coverage and strong surveillance remain critical to preventing international imported measles cases from causing a resurgence of measles in the United States. References
* Three or more cases in a single chain of transmission. Figure 1 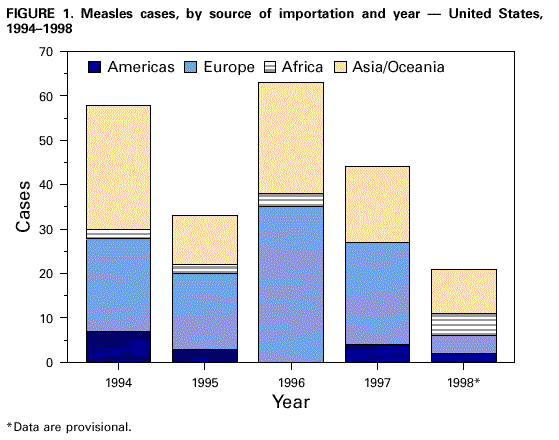 Return to top. Figure 2 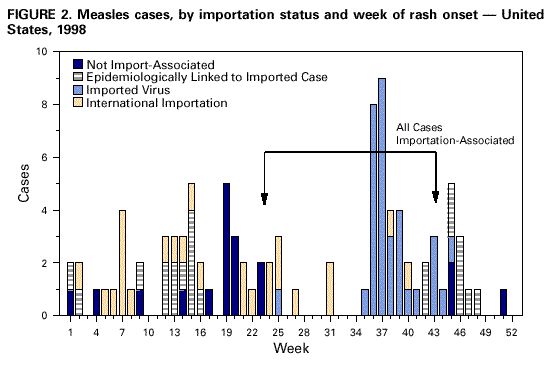 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/2/1999 |
|||||||||
This page last reviewed 5/2/01
|