 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Notice to Readers: Recommended Childhood Immunization Schedule -- United States, 2000Each year, CDC's Advisory Committee on Immunization Practices (ACIP) reviews the recommended childhood immunization schedule to ensure it remains current with changes in manufacturers' vaccine formulations, revisions in recommendations for the use of licensed vaccines, and recommendations for newly licensed vaccines. This report presents the recommended childhood immunization schedule for 2000 (Figure 1) and explains the changes that have occurred since January 1999. Since the publication of the immunization schedule in January 1999 (1), ACIP, the American Academy of Family Physicians, and the American Academy of Pediatrics have recommended removal of rotavirus vaccine from the schedule, endorsed an all-inactivated poliovirus vaccine (IPV) schedule for polio vaccination, recommended exclusive use of acellular pertussis vaccines for all doses of the pertussis vaccine series, and added hepatitis A vaccine (Hep A) to the schedule to reflect its recommended use in selected geographic areas (2). Detailed recommendations for using vaccines are available from the manufacturers' package inserts, ACIP statements on specific vaccines, and the 1997 Red Book (3). ACIP statements for each recommended childhood vaccine can be viewed, downloaded, and printed at CDC's National Immunization Program World-Wide Web site, http://www.cdc.gov/nip/publications/acip-list.htm. Removal of Rotavirus Vaccine from the Schedule On October 22, 1999, ACIP recommended that Rotashield®* (rhesus rotavirus vaccine-tetravalent [RRV-TV]) (Wyeth Laboratories, Inc., Marietta, Pennsylvania), the only U.S. licensed rotavirus vaccine, no longer be used in the United States (4). The decision was based on the results of an expedited review of scientific data presented to ACIP by CDC. Data from the review indicated a strong association between RRV-TV and intussusception among infants 1-2 weeks following vaccination. Vaccine use was suspended in July pending the ACIP data review. Parents should be reassured that children who received the rotavirus vaccine before July are not at increased risk for intussusception now. The manufacturer withdrew the vaccine from the market in October. Inactivated Poliovirus Vaccine for All Four Doses As the global eradication of poliomyelitis continues, the risk for importation of wild-type poliovirus into the United States decreases dramatically. To eliminate the risk for vaccine-associated paralytic poliomyelitis (VAPP), an all-IPV schedule is recommended for routine childhood vaccination in the United States (5). All children should receive four doses of IPV: at age 2 months, age 4 months, between ages 6 and 18 months, and between ages 4 and 6 years. Oral poliovirus vaccine (OPV), if available, may be used only for the following special circumstances:
OPV supplies are expected to be very limited in the United States after inventories are depleted. ACIP reaffirms its support for the global eradication initiative and use of OPV as the vaccine of choice to eradicate polio where it is endemic. Acellular Pertussis Vaccine ACIP recommends exclusive use of acellular pertussis vaccines for all doses of the pertussis vaccine series. The fourth dose may be administered as early as age 12 months, provided 6 months have elapsed since the third dose and the child is unlikely to return at 15-18 months. Hepatitis A Hepatitis A vaccine (Hep A) is listed on the schedule for the first time because it is recommended for routine use in some states and regions. Its appearance on the schedule alerts providers to consult with their local public health authority to learn the current recommendations for hepatitis A vaccination in their community. Additional information on the use of Hep A can be found in recently published guidelines (2). Hepatitis B Special considerations apply in the selection of hepatitis B vaccine products for the dose administered at birth (6). Vaccine Information Statements The National Childhood Vaccine Injury Act requires that all health-care providers, whether public or private, give to parents or patients copies of Vaccine Information Statements before administering each dose of the vaccines listed in this schedule (except Hep A). Vaccine Information Statements, developed by CDC, can be obtained from state health departments and CDC's World-Wide Web site, http://www.cdc.gov/nip/publications/VIS. Instructions on use of the Vaccine Information Statements are available from CDC's website or the December 17, 1999, Federal Register (64 FR 70914). References
* Use of trade names and commercial sources is for identification only and does not constitute or imply endorsement by CDC or the U.S. Department of Health and Human Services. Figure 1 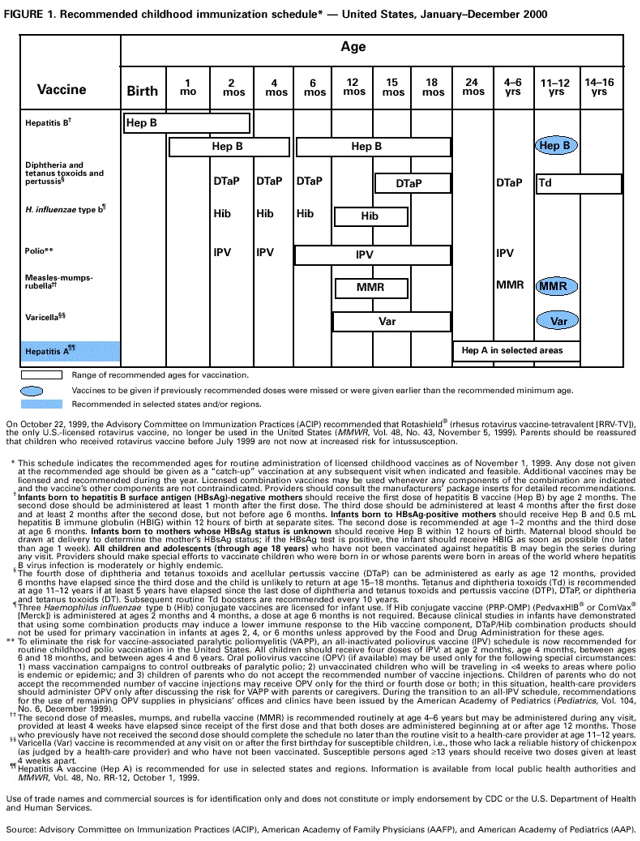 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 1/20/2000 |
|||||||||
This page last reviewed 5/2/01
|