 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. HIV/AIDS Among Men Who Have Sex With Men and Inject Drugs --- United States, 1985--1998Men who have sex with men and inject drugs (MSM/IDU) pose unique challenges for human immunodeficiency virus (HIV) risk reduction efforts because they have multiple risks for HIV acquisition and transmission. This report presents 1) the demographic characteristics of MSM/IDU diagnosed with acquired immunodeficiency syndrome (AIDS) in 1998 and MSM/IDU living with AIDS as of December 31, 1998; 2) trends in AIDS incidence among MSM/IDU from 1985 to 1998; and 3) information on selected behaviors from interviews of MSM/IDU who had AIDS diagnosed from 1996 to 1998 in 12 states.* The findings indicate that 1) over half of MSM/IDU with AIDS were non-Hispanic blacks and Hispanics, and most MSM/IDU with AIDS were reported from large metropolitan statistical areas (MSAs); 2) AIDS incidence has declined since 1996; and 3) a high prevalence of drug-related and sexual risk behaviors occurred among MSM/IDU with AIDS. Demographic and risk characteristics of MSM/IDU aged >13 years with AIDS reported to CDC were obtained from AIDS surveillance data in the 50 states, the District of Columbia, and all U.S. territories. Risk information for AIDS surveillance generally was obtained from medical records. For this analysis, only persons with the reported dual risk factors for HIV transmission of male-male sex and injecting-drug use were included. AIDS diagnoses were adjusted for reporting delays on the basis of cases reported to CDC through December 1999, and for the anticipated reclassification of cases initially reported without risk (1,2). Information on selected behavioral characteristics of MSM/IDU with AIDS was obtained from the Supplement to HIV/AIDS Surveillance (SHAS) project (3). SHAS is a cross-sectional interview study aimed at extending information routinely collected in AIDS surveillance. Persons aged >18 years recently reported with HIV/AIDS to the 12 health departments participating in SHAS were interviewed about their sexual and drug-related risk behaviors. Interview data are presented for men who were classified as MSM/IDU on the HIV/AIDS case report or who reported male-male sex and injecting-drug use in the SHAS interview. Trends Among MSM/IDUThe proportion of all AIDS cases among MSM/IDU decreased from 8% in 1990 to 5% in 1998; 2161 MSM/IDU had AIDS diagnosed in 1998, and 18,133 MSM/IDU were living with AIDS as of December 1998 (Table 1). Most were diagnosed in large MSAs (>1,000,000 persons) and in the South and West.† Non-Hispanic blacks and Hispanics accounted for more than half of each group. AIDS incidence among MSM/IDU increased steadily from 1985 to 1992, and peaked during 1992--1993 (Figure 1), corresponding with the 1993 expansion of the AIDS surveillance case definition. AIDS incidence declined 37% from 1996 to 1998. Interviews of MSM/IDUA total of 513 MSM/IDU who had AIDS diagnosed during 1996--1998 were interviewed for the SHAS project. Of these, 435 (85%) were aged 30--49 years. Non-Hispanic blacks, non-Hispanic whites, and Hispanics accounted for 36%, 42%, and 17%, respectively; Asians/Pacific Islanders and American Indians/Alaska Natives accounted for <2%. The South and the West accounted for 42% and 51% of respondents, respectively, reflecting the geographic distribution of SHAS sites. MSM/IDU interviewed in SHAS had high rates of high-risk sexual and drug-related risk behaviors (Table 2). Eighty-two percent of MSM/IDU had ever used noninjecting drugs, and 61% of MSM/IDU had ever used crack cocaine. Of those injecting drugs during the 5 years preceding the interview, 45% had shared needles. Seventy-six percent of MSM/IDU had sex with men during the 5 years preceding the interview, and 43% had sex with women. Nearly half of those who had sex during the year preceding the interview did not always use condoms. However, consistent condom use was higher when the steady sex partner was known to be uninfected: 61% who had vaginal intercourse, 57% who had insertive anal intercourse with a man, and 61% who had receptive anal intercourse with a man during the year preceding the interview said that they had always used condoms. During the 5 years preceding interview, 18%--20% of MSM/IDU exchanged sex for money or drugs. To assess the degree to which multiple risks are captured in AIDS surveillance, risk classification of the MSM/IDU interviewed in SHAS was examined in AIDS surveillance. Of the 513 MSM/IDU, 352 (69%) were classified as MSM/IDU in AIDS surveillance, 106 (21%) were classified as MSM, 50 (10%) were classified as IDU, and two (0.4%) were classified as having had heterosexual contact or contact with an adult with hemophilia. Reported by: State and territorial health departments; Div of HIV/AIDS Prevention--Surveillance and Epidemiology, National Center for HIV, STD, and TB Prevention; and an EIS Officer, CDC. Editorial Note:The findings in this report document continued declines in AIDS incidence among MSM/IDU since 1996, which resulted in large part from increased use of antiretroviral therapies that delay disease progression (4) and also reflect earlier decreases in HIV incidence among MSM/IDU. The supplemental interview information in a sample of MSM/IDU with AIDS indicates a high prevalence of drug-related and sexual risk behaviors, including sex with men and women. Previous studies have reported similar findings (5,6). Differences in the racial/ethnic, age, and regional distribution of incident and prevalent AIDS cases reflect some differences in historical patterns of HIV incidence. Those include the later onset of the HIV epidemic in the South compared with the West and the Northeast, and the increasing impact on racial/ethnic minorities (7,8). In addition, differences in AIDS incidence and prevalence may reflect differential access to or use of effective antiretroviral treatments. Integrated surveillance for HIV infection and AIDS characterizes persons more recently infected with HIV (9). Non-Hispanic black and Hispanic men were overrepresented among MSM/IDU, accounting for half of MSM/IDU living with AIDS but 22% of the general male population. Race/ethnicity is not a risk factor for HIV infection; social and economic factors associated with race/ethnicity, such as high poverty rates and unemployment and lack of access to health care, are associated with high rates of risk behavior (10). Behavioral risk information for HIV is important to assure that state/local prevention programs are directed to appropriate populations. If providers do not elicit this information or are reluctant to question patients about their sexual and drug-using behaviors, then information in medical records may underrepresent true risks for HIV in the population. Data from the SHAS interviews show that the AIDS surveillance system may have underestimated the number of MSM/IDU and that the true proportion of AIDS cases attributable to MSM/IDU in 1998 may be 7%. Because MSM/IDU have multiple risks for HIV infection, they are particularly vulnerable to infection and can transmit HIV across multiple populations, including MSM, IDU, and heterosexual women. Prevention strategies must provide the information, skills, and support necessary to reduce both sexual and drug-related risk behaviors among MSM/IDU, and include access to drug treatment and to prevention case management. Additional research is needed to determine whether risk reduction strategies that have been effective for groups with single risks also are effective for groups with multiple risks. HIV/AIDS disease surveillance supplemented with behavioral surveys will help in planning prevention, treatment, and other services needed to reduce transmission and to improve survival and quality of life for infected persons. References
*Arizona, California, Colorado, Connecticut, Delaware, Florida, Georgia, Michigan, New Jersey, New Mexico, South Carolina, and Washington. †South=Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia; and West=Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. Table 1 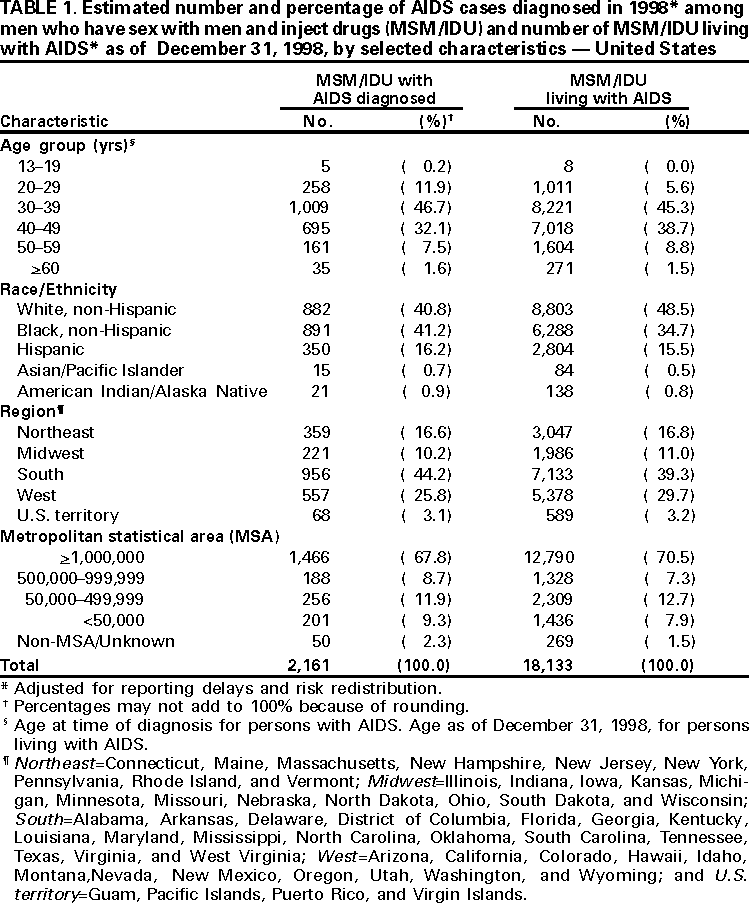 Return to top. Figure 1 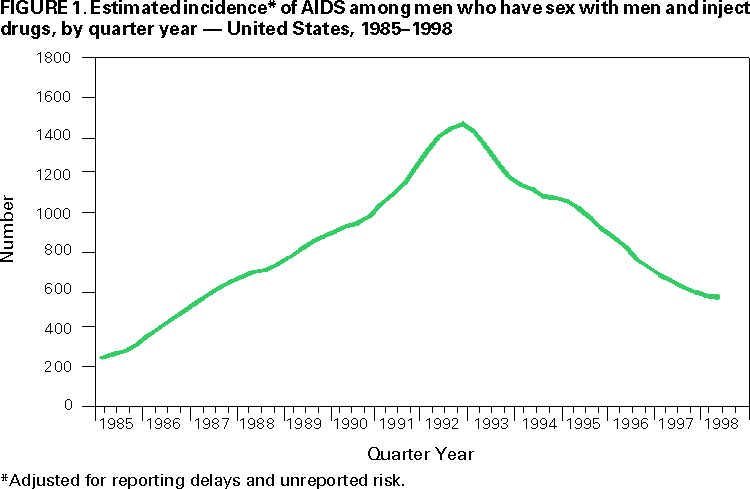 Return to top. Table 2 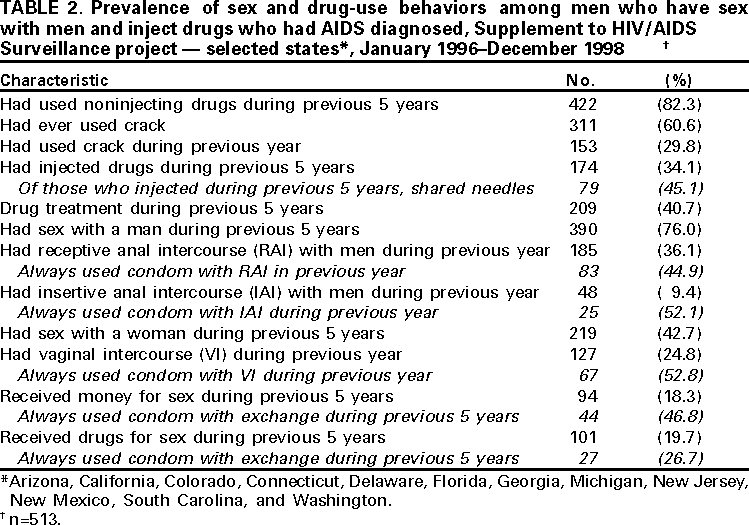 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/5/2000 |
|||||||||
This page last reviewed 5/2/01
|