|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
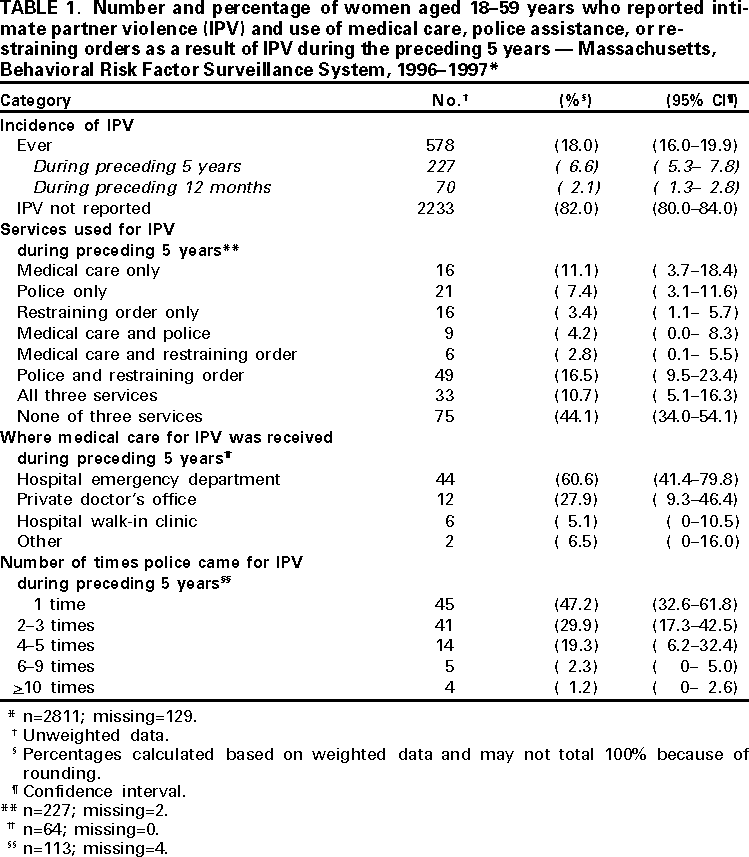
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Use of Medical Care, Police Assistance, and Restraining Orders by Women Reporting Intimate Partner Violence --- Massachusetts, 1996--1997Approximately 1.5 million women in the United States are physically or sexually assaulted by an intimate partner (IP) each year (1). The Woman Abuse Tracking in Clinics and Hospitals (WATCH) Project at the Massachusetts Department of Public Health analyzed data from the 1996 and 1997 Behavioral Risk Factor Surveillance System (BRFSS) in Massachusetts to 1) estimate the percentage of women aged 18--59 years experiencing intimate partner violence (IPV) who used medical care, police assistance, and restraining orders during the preceding 5 years, 2) determine where women experiencing IPV went for medical care, and 3) examine the overlap in use of these three services. This report describes the results of these analyses, which indicate that a higher percentage of women aged 18--59 years use police assistance rather than obtain a restraining order or seek medical care. BRFSS is an ongoing, state-based, random-digit-dialed telephone survey of the U.S. civilian, noninstitutionalized population aged >18 years. Questions on IPV developed by the WATCH Project were added to the Massachusetts BRFSS in 1996 and 1997. During the 2 years, 2940 women aged 18--59 years responded to the survey (response rate: 64.5%). Of these, 129 (5.5%) were excluded from analysis because they either refused or responded "don't know/not sure" to the initial questions about whether they had ever been physically or sexually hurt, and if so, if this was by an IP*. Women aged >60 years also were excluded from the analyses because of low levels of reporting recent IPV. Data were aggregated across the 2 years and weighted to reflect the probability of selection and the demographic distribution of the Massachusetts adult population. Estimated proportions and standard errors were calculated using SUDAAN (2). Survey respondents were asked whether they had ever been physically or sexually hurt† by an IP and when this violence last occurred. Respondents who reported IPV during the preceding 5 years also were asked the following questions about service use: 1) "Did you see a doctor or nurse as a result of being hurt by any of these people in the past five years?"; 2) "In the past five years, were the police called about any of these incidents?"; and 3) "In the past five years, have you gotten a restraining order at a court against a current or ex-(husband/wife), partner, boyfriend, girlfriend, or date?"§ Respondents who reported having seen a doctor or nurse were asked where they sought care most recently, and those who reported police assistance were asked how many times the police had come for incidents of IPV during the preceding 5 years. Among women aged 18--59 years, 18.0% reported ever having experienced IPV, 6.6% reported IPV during the preceding 5 years, and 2.1% reported IPV during the preceding 12 months (Table 1). Among women reporting IPV during the preceding 5 years, 39.0% received police assistance, 33.8% obtained a restraining order, and 28.7% sought medical care as a result of IPV. Most women who received police assistance also reported obtaining a restraining order: 69.7%¶ of women who received police assistance for IPV also obtained a restraining order against an IP. Among women reporting IPV, 11.1% sought medical care as a result of IPV but did not obtain police assistance or a restraining order. Approximately half (55.9%) of women reporting IPV received one or more of the three services. Most women reporting IPV during the preceding 5 years were aged 18--29 years (64.0%), employed (69.8%), had some college education (60.3%), and had children in the household (52.5%). Half (50.1%) of women had never been married, 28.6% were divorced or separated, and 21.3% were married or cohabitating. Reported by: J Hathaway, MD, J Silverman, PhD, G Aynalem, MD, Woman Abuse Tracking in Clinics and Hospitals Project, Bur of Family and Community Health; L Mucci, MPH, D Brooks, MPH, Chronic Disease Surveillance, Bur of Health Statistics, Research and Evaluation, Massachusetts Dept of Public Health. Family and Intimate Violence Prevention Team, Div of Violence Prevention, National Center for Injury Prevention and Control, CDC. Editorial Note:Federal, state, and local efforts are under way to establish surveillance systems for IPV. The WATCH Project, along with projects in Michigan and Rhode Island, have been funded by CDC to establish statewide tracking systems for IPV against women. IPV surveillance systems are frequently based on service provider data; however, these data represent only persons accessing that particular service. Service provider data are unable to provide estimates of the total number of women experiencing IPV in a population or the extent to which the same women may be represented in different service provider data sets. Surveillance data from the WATCH Project provide state-based estimates of the percentage of women experiencing IPV using three key types of services and the degree of overlap in service use. Other population-based studies report similar findings regarding the frequency at which women experiencing IPV use services. Police assistance for IPV is received by 35%--56% of women reporting IPV (3--5). Of women physically abused by their partners, 22% seek restraining orders against an IP (4). Among women reporting IPV, 10%--21% receive medical care as a result of IPV, and approximately 70% of these police and restraining order and the percentage who used police, restraining order, and medical care divided by the percentage who used police with or without other services. women seek care at an emergency department (3,4,6). Finally, 16% of persons who experience family violence or IPV identified through police incident reports have violence-related contact with a regional hospital (7). The findings in this report are subject to at least three limitations. First, BRFSS is a retrospective self-report survey and may be subject to recall bias. Second, women experiencing IPV who were not eligible to be included in the phone survey, declined participation, or did not disclose IPV may have a different pattern of service use than respondents. Persons who were ineligible to participate included those who were homeless, lived in group housing, did not have a phone, or did not speak English, Spanish, or Portuguese. Finally, IPV may not have been reported because of mistrust, fear of reprisals, and feelings of shame and/or denial. These findings have implications for both IPV surveillance and medical practice. For surveillance, these results suggest that police data may capture a larger portion of women aged 18--59 years experiencing IPV than a medical care-based surveillance system. In Massachusetts, where police are directed to inform women reporting IPV about the availability of restraining orders, police and restraining order data appear to capture a similar demographic group. However, a medical care-based tracking system may capture a sizeable portion of women experiencing IPV who do not receive police or restraining order assistance. Emergency departments appear to provide the most efficient location within the medical system for tracking IPV-related injuries because most women who seek medical care following incidents of IPV are seen in emergency departments. However, a surveillance system designed to include police, restraining order, and medical care data may miss nearly half of women experiencing IPV. Medical practitioners, particularly those in emergency departments, need to be prepared to identify and provide support, safety planning, and resources to those experiencing IPV (8). Because many women experiencing IPV do not disclose partner violence unless directly asked, some groups believe women patients whose conditions may be injury-related should be screened systematically for IPV (9,10). Because 38.7% of women who received medical care for IPV had not received police or restraining order assistance, medical practitioners may be a critical source of support and intervention to many women. References
* Same or opposite sex, current or ex-husband/wife, partner, boyfriend, girlfriend, or date. † Being physically or sexually hurt included being shoved, slapped, hit with an object, or forced into any sexual activity. § Questions on medical care and restraining orders were revised during 1996-1997 for clarification. The question on medical care was reworded from "after being hurt" to "as a result of being hurt" and the question on restraining orders was reworded from "have you been to court to get a restraining order" to "have you gotten a restraining order at a court." Response frequencies for women aged 18-59 years did not vary significantly for each version of the question. ¶ Calculated as the percentage of women who used police and restraining order and the percentage who used police, restraining order, and medical care divided by the percentage who used police with or without other services.Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/8/2000 |
|||||||||
This page last reviewed 5/2/01
|