|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
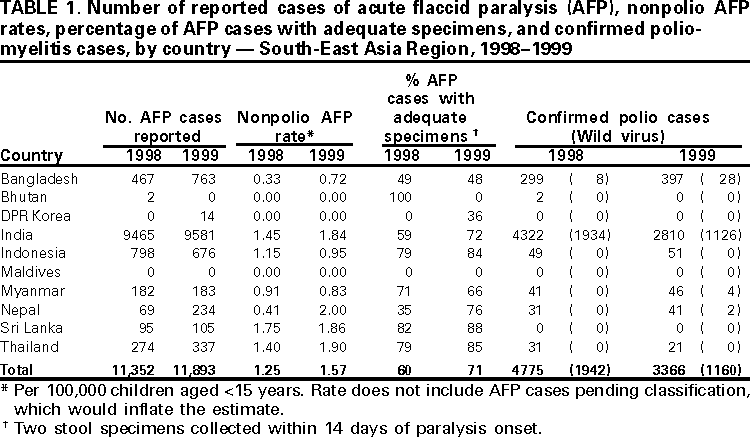
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- South-East Asia Region, 1998--1999In 1988, the World Health Assembly resolved to eradicate poliomyelitis by the end of 2000 (1). To achieve this goal, the 10 member countries* of the World Health Organization (WHO) South-East Asia Region (SEAR) began implementing polio eradication strategies in 1994. In 1999, most polio cases worldwide were reported in SEAR (i.e., 48% of reported polio cases and 62% of cases with wild poliovirus isolation) (2,3). This report summarizes progress in achieving high routine and supplemental vaccination coverage, the surveillance of cases of acute flaccid paralysis (AFP), and the impact of these activities on polio eradication in the region during 1998--1999. Routine VaccinationIn 1998, four countries reported coverage of >80% with three doses of oral poliovirus vaccine (OPV3); five countries reported coverage of 73% to 78%. In 1999, seven countries reported coverage of >90%. However, in India during 1997--1998, surveys indicated that OPV3 coverage varied markedly at the state and city level; coverage in many areas was <50% (4). Supplementary VaccinationIn 1999, all SEAR countries conducted supplemental OPV vaccination activity. On the basis of recommendations from the Technical Consultative Group on Poliomyelitis Eradication (5), India conducted four rounds of National Immunization Days (NIDs)† from October 1999 to January 2000 and two rounds of Subnational Immunization Days (SNIDs)§ during February--March 2000 in eight high-risk northern states. In 1999, the largest public health campaign ever conducted in one country took place in India, where one NID round reached 147 million children aged <5 years. Bangladesh, Bhutan, DPR Korea, Maldives, Myanmar, Nepal, Sri Lanka, and Thailand held two rounds of NIDs. Bangladesh completed NIDs during November--December 1999, and conducted SNIDs. Indonesia and Myanmar conducted mopping-up¶ campaigns, and India and Bangladesh added a house-to-house component to their NIDs and Nepal to its SNIDs. Synchronizing with India, Nepal held its NIDs during November--December 1999 and its SNIDs during January--February 2000. AFP SurveillanceAFP surveillance is conducted to identify the remaining infected areas, to target supplemental vaccination, and to monitor progress toward eradication through a network of reporting units dispersed throughout a country. WHO recommends immediately reporting and investigating every AFP case in children aged <15 years within 48 hours after notification, and collecting two stool samples for analysis in a WHO-accredited laboratory (6). AFP surveillance is evaluated by the sensitivity of reporting (i.e., nonpolio AFP rate of at least one case per 100,000 children aged <15 years) and the completeness of specimen collection (i.e., two adequate stool specimens from at least 80% of persons with AFP). In SEAR countries where polio is endemic, AFP surveillance was strengthened using surveillance medical officers (SMOs) who receive special training and are responsible for a defined area. From 1998 to 1999, the number of SMOs increased in Bangladesh from zero to 16, in India from 59 to 108, and in Nepal from four to six. Since 1999, AFP surveillance in Bangladesh, India, and Nepal also has been supported through the use of Stop the Transmission of Polio (STOP) teams**. With the addition of SMOs and STOP teams, the number of reported AFP cases increased in Bangladesh from 467 in 1998 to 763 in 1999, and in Nepal from 69 in 1998 to 234 in 1999 (Table 1). In 1999, India, Sri Lanka, and Thailand had nonpolio AFP rates of >1.0, and Nepal had a nonpolio AFP rate of >1.0 for the first time. In Indonesia, nonpolio AFP rates decreased from 1.15 in 1998 to 0.95 in 1999. AFP surveillance in DPR Korea started in 1999, and 14 AFP cases were reported. In 1998 and 1999, the proportion of AFP cases with adequate stool specimens was 82% and 88% in Sri Lanka, 79% and 85% in Thailand, 79% and 84% in Indonesia, 35% and 76% in Nepal, 59% and 72% in India, 71% and 66% in Myanmar, 49% and 48% in Bangladesh, and 0% and 36% in DPR Korea, respectively. Polio Laboratory NetworkIn 1999, 14 of 17 network laboratories performing primary virus isolation from stool specimens were fully WHO-accredited. One laboratory in Jakarta, Indonesia, was accredited provisionally and the two remaining laboratories (Dhaka, Bangladesh; and Pyongyang, DPR Korea) are being strengthened for accreditation review. Four network laboratories are regional reference laboratories and perform intratypic differentiation (wild poliovirus versus vaccine-derived virus) of isolated polioviruses. The overall number of stool specimens processed by these laboratories increased from 3376 in 1997 to 22,657 in 1999. Polio IncidenceIn India, the overall number of reported polio cases decreased from 4322 (1934 virus-confirmed) in 1998 to 2810 (1126 virus-confirmed) in 1999 (Table 1). Most of the decrease in virus-confirmed cases occurred in central and southern Indian states; no substantial decrease was reported in the high-risk northern states of Bihar, Delhi, Uttar Pradesh, or West Bengal. Of 1138 wild polioviruses isolated in India in 1999, 730 (64%) were poliovirus type 3 and 397 (35%) were poliovirus type 1. India, the only country reporting poliovirus type 2 in 1999, indicated a decrease from 83 cases in 1998 to 11 in 1999 (10 in Uttar Pradesh and one in West Bengal). The overall number of polio cases reported from Bangladesh increased from 299 (eight virus-confirmed) in 1998 to 397 (28 virus-confirmed) in 1999. Myanmar and Nepal reported no cases of wild poliovirus during 1998. However, wild poliovirus was reported from both countries in 1999; Nepal reported two cases from its border with India (Uttar Pradesh) (7), and Myanmar reported four cases from its border with Bangladesh (8). The Myanmar cases represent virus importation from Bangladesh because the cases were found close to the border, and the isolated virus showed more genetic similarity with virus isolated in Bangladesh than with indigenous Myanmar virus. In 1999, Bhutan, DPR Korea, Maldives, and Sri Lanka reported no polio cases. Indonesia and Thailand reported clinically confirmed cases but no virologically confirmed wild poliovirus cases. Reported by: Vaccines and Biologicals Dept, World Health Organization, Regional Office for South-East Asia, New Delhi, India. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Respiratory and Enterovirus Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:Approximately 25% of the world's population live in SEAR countries, most in India, the largest country where polio is endemic (population: 1 billion). Progress in this region is critical for the success of global polio eradication. Although large numbers of polioviruses 1 and 3 circulated in 1999, transmission occurred mainly in four states in northern India, with focal transmission of poliovirus 2 limited to two of these states. Transmission of virus in southern India decreased substantially from 1998 to 1999. Virologically confirmed wild poliovirus cases found in border districts in Myanmar and Nepal highlight the importance of border regions in the transmission of wild poliovirus and the need for cooperation of neighboring countries in surveillance and planning of NIDs. In 1999, a cross-border collaboration meeting was held between Bangladesh, India, and Nepal. Surveillance in Bangladesh and Nepal improved when additional SMOs and STOP teams were assigned to the program. Surveillance in DPR Korea needs improvement. India accounts for 40% of confirmed polio cases and 60% of wild poliovirus isolates worldwide. During 2000, four, three, and two extra NIDs rounds will be conducted in the high-risk, medium-risk, and low-risk states, respectively. Aggressive mopping-up activities also will be carried out. Bangladesh and Nepal plan to conduct extra NIDs rounds with an increased proportion of vaccine to be delivered house-to-house. If these supplemental activities reach a high proportion of the target population in Bangladesh, India, and Nepal (the remaining countries of the region where polio is endemic) poliovirus transmission could be interrupted in these countries by the end of 2000 or soon after. References
† Nationwide, mass campaigns over a short period (days to weeks) in which two doses of OPV are administered to all children, usually aged <5 years, regardless of vaccination history, with an interval of 4--6 weeks between doses. § Subnational Immunization Days (SNIDs) follow the same procedure as NIDs but on a regional level. ¶ Focal mass campaigns in high-risk areas over a short period (days to weeks) in which two doses of OPV are administered during house-to-house and boat-to-boat visits to all children aged <5 years, regardless of vaccination history, with an interval of 4--6 weeks between doses. ** Groups of international health professionals deployed to a district for 3 months to assist ministry of health staff with polio eradication activities. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/29/2000 |
|||||||||
This page last reviewed 5/2/01
|