 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Cigarette Smoking Among Adults --- United States, 1998One of the national health objectives for 2010 is to reduce the prevalence of cigarette smoking among adults to no more than 12% (objective 21.1a) (1). To assess progress toward meeting this objective, CDC analyzed self-reported data from the 1998 National Health Interview Survey (NHIS) Sample Adult Core Questionnaire about cigarette smoking among U.S. adults. This report summarizes the findings of this analysis, which indicate that, in 1998, 24.1% of adults were current smokers. The 1998 NHIS Core Questionnaire was administered to a nationally representative sample (n=32,440) of the U.S. noninstitutionalized civilian population aged >18 years; the overall response rate for the survey was 73.9%. Participants were asked, "Have you smoked at least 100 cigarettes in your entire life?" and "Do you now smoke cigarettes every day, some days, or not at all?" Current smokers were persons who reported both having smoked >100 cigarettes during their lifetime and having smoked every day or some days at the time of the interview. Former smokers were those who had smoked >100 cigarettes during their lifetime but did not currently smoke. Attempts to quit were determined by asking current smokers, "During the past 12 months, have you stopped smoking for one day or longer because you were trying to stop smoking?" Data were adjusted for nonresponse and weighted to provide national estimates. Confidence intervals (CIs) were calculated using SUDAAN. In 1998, an estimated 47.2 million adults (24.1%), comprising 24.8 million men (26.4%) and 22.4 million women (22.0%), were current smokers (Table 1). Overall, 19.7% (95% CI=±0.6) of adults were everyday smokers, and 4.2% (95% CI=±0.3) were someday smokers (everyday smokers constituted 82.4% [95% CI=±1.0] of all smokers). Prevalence of smoking was highest among persons aged 18--24 years (27.9%) and aged 25--44 years (27.5%), and lowest among persons aged >65 years (10.9%). Prevalence of current smoking was highest among American Indians/Alaska Natives (40.0%), intermediate among non-Hispanic whites (25.0%) and non-Hispanic blacks (24.7%), and lowest among Hispanics (19.1%) and Asians/Pacific Islanders (13.7%). Adults with >16 years of education had the lowest smoking prevalence (11.3%), achieving the 2010 goal of reducing smoking rates to no more than 12%. Current smoking prevalence was highest among persons with 9--11 years of education (36.8%). Smoking prevalence was higher among persons living below the poverty level* (32.3%) than among those living at or above the poverty level (23.5%). In 1998, an estimated 44.8 million adults (22.9% [95% CI=±0.6]) were former smokers, comprising 25.7 million men and 19.1 million women. Former smokers constituted 48.7% (95% CI=±1.0) of persons who had ever smoked >100 cigarettes. Among current daily smokers in 1998, an estimated 15.2 million (39.2% [95% CI=±1.4]) had stopped smoking for at least 1 day during the preceding 12 months because they were trying to stop smoking. Reported by: Epidemiology Br, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report suggest that the goal of reducing the prevalence of cigarette smoking among adults to <12% by 2010 will require aggressive public health efforts to implement comprehensive tobacco-control programs nationwide (2). The 1998 NHIS data also demonstrate substantial differences in smoking prevalence across populations. In 1998, smoking prevalence among persons aged 18--24 years was as high as the prevalence among persons aged 25--44 years. Historically, smoking prevalence has been highest among persons aged 25--44 years and significantly lower among persons aged 18--24 years. Recent increases among persons aged 18--24 years may reflect the aging of the cohort of high school students among whom current smoking rates were high during the 1990s (3). In addition, the increase may indicate increased initiation of smoking among young adults. The high prevalence of smoking among young adults indicates a need to focus tobacco-use prevention and treatment programs on both adolescents and young adults. Smoking prevalence reported for racial/ethnic subgroups showed few changes from 1997 (4) to 1998. Prevalence of current smoking among American Indians/Alaska Natives remained the highest. State and regional surveys indicate that the prevalence of smoking cessation among American Indians/Alaska Natives remains relatively low (5). Although many factors contribute to the high prevalence of smoking among American Indians/Alaska Natives, it is important to develop culturally appropriate prevention and control measures that distinguish between the use of manufactured tobacco products and the ceremonial use of tobacco. National health objectives for 2010 that are focused on eliminating population disparities reinforce the need for greater surveillance and culturally responsive approaches to tobacco use across communities (1). In the United States, population disparities in smoking prevalence have been consistent from 1993 through 1998. For example, in 1993, an 8.3 (95% CI=±2.5) percentage-point difference in smoking prevalence existed between those at or above the poverty level and those below (23.8% and 32.1%, respectively). In 1998, the difference was 8.8 (95% CI=±1.9) percentage points (23.5% and 32.3%, respectively). Similarly, differences in prevalence among various educational groups have not been reduced. In 1993, the difference between those with 9--11 years of education and those with >16 years was 23.3 (95% CI=±3.0) percentage points (36.8% and 13.5%, respectively). In 1998, the difference was 25.5 (95% CI=±2.3) percentage points (36.8% and 11.3%, respectively). The relation between tobacco use and increased risk for failing or dropping out of high school demonstrates the necessity of reaching these students (6) through school-based programs (7,8) before they leave school. Differences in prevalence among racial/ethnic subgroups have not been reduced. For example, in 1993, the difference between non-Hispanic whites and American Indians/Alaska Natives was 13.3 (95% CI=±8.7) percentage points (25.4% and 38.7%, respectively). In 1998, the difference between non-Hispanic whites and American Indians/Alaska Natives was 15.0 (95% CI=±9.8) percentage points (25.0% and 40.0%, respectively). The reduction of tobacco-related health disparities requires communities, states, and national organizations to take a multidisciplinary approach to tobacco prevention and control (7,8). The findings in this report are subject to at least two limitations. Because the questionnaire for the 1997 NHIS was redesigned completely, trend analysis or comparison with data from years before 1997 should be conducted with caution. Second, the sample size of certain subgroups (e.g., American Indians/Alaska Natives) was small, possibly resulting in unstable estimates. Although comprehensive programs are critical in reducing the burden of tobacco use, short-term decreases in tobacco-related morbidity and mortality can be achieved only by helping current smokers quit. To assist in this process, the U.S. Department of Health and Human Services has released guidelines (9) with specific evidence-based recommendations for tobacco-use treatment. Recommended interventions include individual, group, or telephone counseling that offers practical advice about and support for quitting; support from family and friends also improves success rates. In addition, all smokers trying to quit should be encouraged to use a medication approved by the Food and Drug Administration, either nicotine replacement therapy (gum, inhaler, nasal spray, or patch) or a non-nicotine pharmacologic aid (buproprion). To ensure that smokers interested in quitting receive appropriate treatment, health-care systems must make routine screening of tobacco use the standard of care and monitor (through quality assurance processes) the provision of appropriate interventions to smokers. Improving access to treatment by reducing cost barriers also increases the number of quitters. A comprehensive approach to tobacco control will require treatment for nicotine dependence and efforts at national, state, and local levels to reduce youth smoking, promote smoke-free environments, support countermarketing efforts, enforce laws and regulations, and eliminate disparities in tobacco use among population subgroups (7,8). Increased attention must be focused on groups that show no decline in smoking prevalence, including persons aged 18--24 years, adults with low education levels, and American Indians/Alaska Natives. Approaches with the widest scope (i.e., economic, regulatory, and comprehensive) are likely to have the greatest long-term population impact (10). References
*1997 poverty thresholds from the Bureau of the Census, Economics and Statistics Administration, U.S. Department of Commerce, were used in these calculations. Table 1 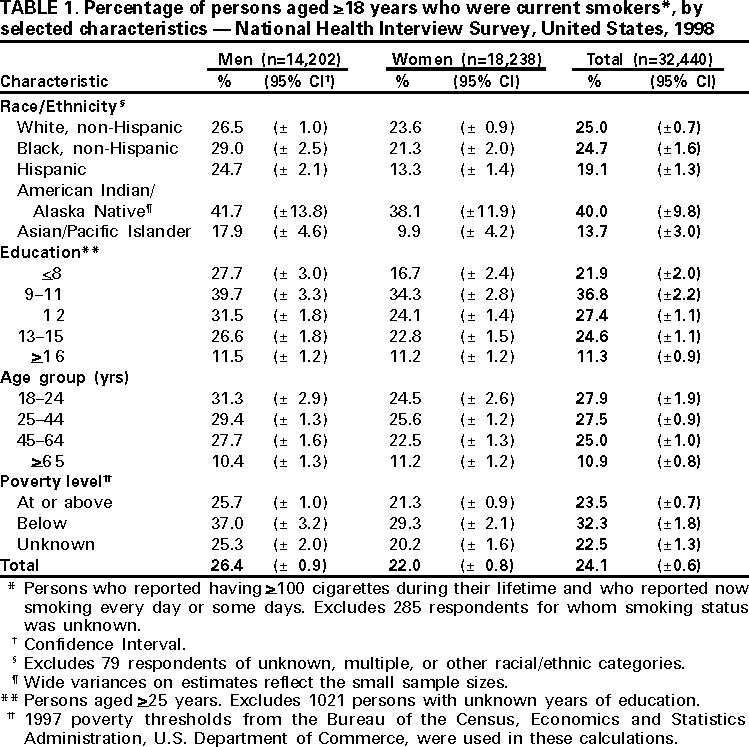 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/5/2000 |
|||||||||
This page last reviewed 5/2/01
|