 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Rift Valley Fever --- Saudi Arabia, August--October, 2000Please note: An erratum has been published for this article. To view the erratum, please click here. On September 10, 2000, the Ministry of Health (MOH), Kingdom of Saudi Arabia, and subsequently the Ministry of Health of Yemen received reports of unexplained hemorrhagic fever in humans and associated animal deaths from the southwestern border of Saudi Arabia and Yemen. Signs and symptoms of ill persons included low grade fever, abdominal pain, vomiting, diarrhea, jaundice with liver and renal dysfunction often progressing to disseminated intravascular coagulation, hepatorenal syndrome, and death. On September 15, using ELISA (antigen detection and IgM), polymerase chain reaction, virus isolation, and immunohistochemistry, CDC confirmed the diagnosis of Rift Valley fever (RVF) in all four serum samples submitted from Saudi Arabia. This report summarizes the preliminary results of the collaborative epidemiologic investigation performed by the Saudi Arabian MOH, CDC, and the National Institute of Virology, South Africa, of the first confirmed occurrence of RVF outside Africa. As of October 9 in Saudi Arabia, 316 persons with suspected severe RVF* have been reported from primary health-care centers and hospitals. All suspected severe cases have been hospitalized for care and management. Of the 316 case-patients, 245 (78%) were male; the median age was 46 years (range: 11--95 years); 15 (5%) were aged <16 years; 253 (80%) were Saudi citizens and 63 (20%) were Yemen citizens. At least 66 (21%) patients have died. Suspected severe case-patients investigated to date resided in or visited the floodplains of the wadis (i.e., seasonal riverbeds) that emanate from the foothills of the Sarawat mountains and extend south of Jeddah to the border of Yemen (Figure 1). Of the 316 suspected cases, 304 (96%) have been reported from the southern coastal province of Jizan (1992 population: 860,000) and the contiguous Asir and Al Quenfadah health regions. Cases from four other health regions have documented travel to these areas. The onset of the earliest suspected case was August 27 (Figure 2). The activities of the MOH, Ministry of Agriculture and Water, and Ministry of Municipalities to contain the outbreak included an intensive mosquito-control program; restriction of movement of domestic animals; a comprehensive educational campaign to eliminate contact with sick animals and mosquitoes (including provision of free permethrin-impregnated bednets); encouragement to seek early medical evaluation of persons with febrile illnesses; and information for health-care providers on the clinical presentation and management of suspected cases. Studies are in progress to identify risk factors for infection, severe disease, and mortality. Animal, human, and vector surveillance is being strengthened throughout the country, including establishment of central human and veterinary virology laboratories in Riyadh and Jizan, respectively. A kingdomwide survey among domestic ungulates, primarily sheep and goats, is under way to define the boundaries for a veterinary vaccination program. Additional studies are planned to assess the magnitude of the outbreak, to define infection rates among high-risk groups, such as veterinarians and slaughterhouse workers, and to determine evidence for nosocomial transmission. Reported by: H Arishi, MD, A Ageel, MD, MA Rahman, MD, AA Hazmi, MD, AR Arishi, MD, B Ayoola, MD, C Menon, MD, J Ashraf, MD, O Frogusin, MD, F Sawwan, M Al Hazmi, MD, King Fahd Central Hospital, Jizan; A As-Sharif, MS, M Al Sayed, A Raheem Ageel, MD, Regional Health Affairs, Jizan; ARA Alrajhi, MD, King Faisal Specialist Hospital and Research Center, Riyadh; MA Al-Hedaithy, MD, College of Medicine, King Khalid Univ Hospital, Riyadh; A Fatani, MBBS, A Sahaly, MBBS, A Ghelani, MBBS, T Al Basam, MBBS, A Turkistani, BDS, N Al Hamadan, MBBS, Saudi Arabia Field Epidemiology Training Program, Riyadh; A Mishkas, MBBS, Infectious Diseases; MH Al-Jeffri, MBBS, Parasitic and Infectious Diseases; YY Al Mazroa, MD, MMA Alamri, MM Al-Qahtani, MBBS, A Al Drees, Laboratories and Blood Banks, Riyadh; T Madden, MD, G Al Gazebo, OA Shubokshi, MD, Ministry of Health, Saudi Arabia. P Jupp, PhD, A Kemp, MS, F Burt, PhD, R Swanepoel, PhD, Pathogens Unit, National Institute of Virology, Johannesburg, South Africa. Infectious Disease Pathology Activity, Special Pathogens Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases, CDC; and an EIS Officer. Editorial Note:RVF is a mosquitoborne zoonotic viral disease predominantly causing abortion and deaths of young animals (e.g., sheep and goats) (1). Epizootic and epidemic transmission is associated with periodic heavy rainfall. Human infection is predominately not apparent or is associated with a brief self-limited febrile illness. However, complications such as retinitis, hemorrhagic fever, or encephalitis occur in some patients (approximately 15%, 1%, and 1%, respectively) (1). Transmission is primarily by contact with infected animal body fluids and mosquito bites, although virology laboratory workers also are at risk. Person-to-person transmission has not been reported. The Saudi Arabian MOH is evaluating the feasibility of a randomized, placebo-controlled trial using intravenous ribavirin in patients with suspected severe RVF. Although ribavirin has not been administered to humans with RVF, evidence suggests its efficacy in animal models (2). Intravenous ribavirin has been shown to treat effectively other viral hemorrhagic fevers, including Lassa fever, hemorrhagic fever with renal syndrome, and Crimean-Congo hemorrhagic fever (2). This outbreak on the Arabian Peninsula represents the first cases of RVF outside Africa. The potential of RVF virus to establish transmission and cause disease in new areas first was documented during its emergence in Egypt in 1977; previously, the disease was limited to sub-Saharan Africa. The virus isolated from the blood of the first patients had a RNA sequence similar to the RVF viruses isolated during 1997--1998 East African outbreaks (3). Cross-sectional community surveys for asymptomatic and milder illnesses and laboratory evidence of infection are in progress to assess the magnitude and geographic extent of infection. References
* Screening case definition for RVF: unexplained illness >48 hours in duration associated with three times elevation in transaminases (aspartate aminotransferase, alanine aminotrans ferase, and gamma glutamyl transpeptidase) or clinical jaundice; or unexplained illness >48 hours in duration associated with abortion or bleeding manifestations (e.g., from puncture sites, ecchymosis, petechiae, purpura, epistaxis, gastrointestinal bleeding, or menorrhagia); or unexplained acute visual loss or scotoma; or unexplained illness >48 hours in duration associated with neurologic manifestations (e.g., vertigo, confusion, disorientation, amnesia, lethargy, hallucination, meningismus, choreiform movements, ataxia, tremor, convulsions, hemiparesis, decerebrate posturing, locked-in syndrome, or coma); or unexplained illness >48 hours in duration associated with fever, diarrhea, nausea, vomiting, or abdominal pain and any one of the following laboratory values: 1) hemoglobin <8 gm/dL; 2) platelets <100,000 mm3 (<10 x 1010/L); 3) LDH 2 x upper limit of normal; 4) creatinine >150 mol/L; 5) CPK 2 x upper limit of normal; or unexplained death with history of fever, lethargy, diarrhea, abdominal pain, nausea, vomiting, or headache in the preceding 2 weeks. Figure 1 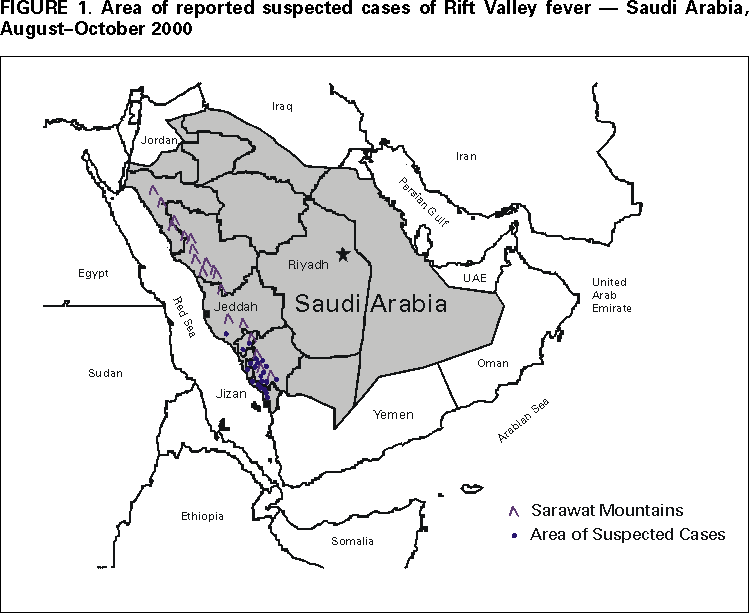 Return to top. Figure 2 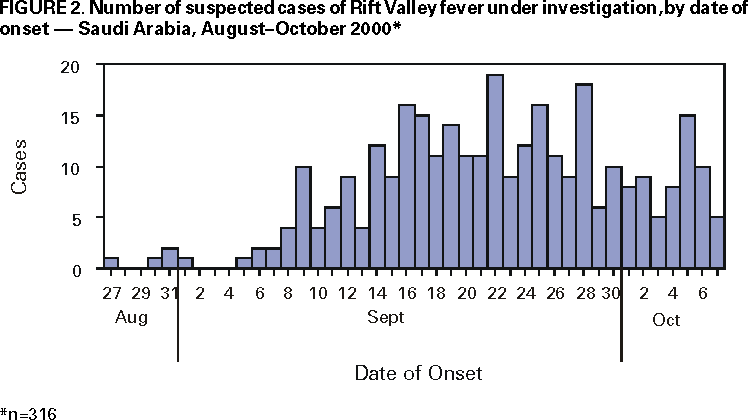 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 10/12/2000 |
|||||||||
This page last reviewed 5/2/01
|