 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Coccidioidomycosis in Travelers Returning From Mexico --- Pennsylvania, 2000Coccidioidomycosis (CM), a fungal disease caused by Coccidioides immitis, is endemic in the southwestern United States and parts of Central and South America. The disease is acquired by inhaling the arthroconidia of C. immitis present in the soil. Outbreaks of CM occur when susceptible persons are exposed to airborne arthroconidia from dust storms, natural disasters, and earth excavation (1,2). Persons who travel to areas where the disease is endemic may become infected and develop symptoms after returning home (3,4). This report describes an outbreak of CM among travelers returning to Pennsylvania from a trip to Mexico. On January 24, 2000, 35 church members from two cities in Pennsylvania traveled to Hermosillo, Mexico, where they stayed 1 week to construct a church. Within 2 weeks of returning home, 27 travelers complained of influenza-like symptoms, and initial testing of acute serum specimens at CDC revealed antibodies to C. immitis for one traveler. To determine the extent of the outbreak and to identify potential risk factors for developing CM, the Pennsylvania Department of Health and CDC conducted a cohort study and collected acute and convalescent-phase serum samples from consenting church members. Serum specimens were tested for antibodies to C. immitis by immuno-diffusion and complement fixation at CDC and the University of California-Davis. A case was defined as a positive serologic test for coccidioidal antibodies by 1) detection of coccidioidal immunoglobulin M by immunodiffusion, enzyme immunoassay (EIA) latex agglutination, or tube precipitin, or 2) detection of rising titer of coccidioidal immuno-globulin G by immunodiffusion, EIA, or complement fixation in a church member from Pennsylvania who had traveled to Hermosillo during January 24--February 2, 2000. All participants completed a standardized questionnaire about medical history, activities while in Mexico, and environmental exposures. A questionnaire and at least one serum sample was obtained for 30 (86%) of the 35 church members. Twenty-nine (97%) were men; median age was 45 years (range: 18--62 years). Twenty-three (77%) persons reported becoming ill either in Mexico or within 3 weeks of returning home. Based on serologic testing, eight (27%) persons met the case definition for CM, seven of whom were symptomatic (Figure 1). The incubation period ranged from 8 days after arriving in Mexico to 15 days after returning to Pennsylvania from Mexico. The most common symptoms were fatigue, fever, arthralgias, and myalgias (71% in each). Three had a rash, and four had a cough. The median duration of symptoms was 7 days (range: two--35). Eighteen (78%) of 23 ill persons sought care from at least one health-care provider. Twelve (67%) persons had chest radiographs performed as part of their evaluation; six were abnormal. Eleven of these 18 persons were prescribed medications for their symptoms; six were prescribed either fluconazole or itraconazole once it was known that a CM outbreak had occurred. One person required hospitalization in an intensive care unit for 1 day. Of 23 ill persons, 11 (48%) missed work or school for an average of 5.5 days. No activities or other conditions were associated substantially with infection or symptomatic disease. However, 22 (73%) church members reported working in extremely dusty conditions. Nineteen (63%) persons reported histories of previous travel to Hermosillo or other areas where C. immitis is endemic; but only one case-patient reported history of such travel. Reported by: J Zurlo, MD, T Crook, MD, W Green, MD, J Adams, MD, Hershey Medical Center, Hershey; C Freer, MD, Hanover Hospital, Hanover; J Ratner, MD, Center Community Hospital, State College; N M'ikanatha, DrPH, J Rankin, DVM, L Stetson, MPH, S Yeager, Pennsylvania Dept of Health. D Pappagianis, MD, Univ of California-Davis, Davis. Mycotic Diseases Br, Div of Bacterial and Mycotic Diseases, National Center for Infectious Diseases; and EIS officers, CDC. Editorial Note:The outbreak in this report and a similar outbreak in a group from Washington (3) underscore the need for increased awareness about CM and its risk factors among susceptible persons visiting areas where the disease is endemic, especially among persons who engage in construction work or other activities in dusty environments. Travel to these areas has become more common because of various missionary and other travel activities to Mexico and relocation of persons from areas in the Northwest and Midwest to the southwestern United States (3--5). In addition, CM has increased among U.S. travelers to areas where CM is endemic, especially among the elderly (6). Persons with certain underlying illnesses (e.g., human immunodeficiency virus [HIV] and elderly with chronic medical conditions) who travel to areas where CM is endemic are at increased risk for severe pulmonary or disseminated CM (7,8). Approximately 40% of persons infected with C. immitis develop symptomatic disease. Most (85%) symptomatic persons present with a mild, influenza-like illness; 8% may develop severe pulmonary disease requiring hospitalization, and 7% develop disseminated, extrapulmonary disease (7). Risk factors for disseminated disease include black or Asian race, pregnancy, and immunocompromising conditions (e.g., acquired immunodeficiency syndrome); risk factors for severe pulmonary disease include diabetes, smoking, and older age (7). Although avoiding activities that generate dust or using a mask during these activities is advisable, these measures do not provide complete protection. A potential strategy for adequate prevention is vaccine development because natural infection with C. immitis provides life-long immunity (9). However, until a vaccine becomes available, organizations that conduct trips to areas where CM is endemic should inform their travelers about the risks for CM. Health-care providers should consider CM in travelers returning from areas where the disease is endemic and who present with an influenza-like illness. Early diagnosis of CM will result in better use of medical resources and will help alleviate patient concerns and may prevent more severe disease (7). References
Figure 1 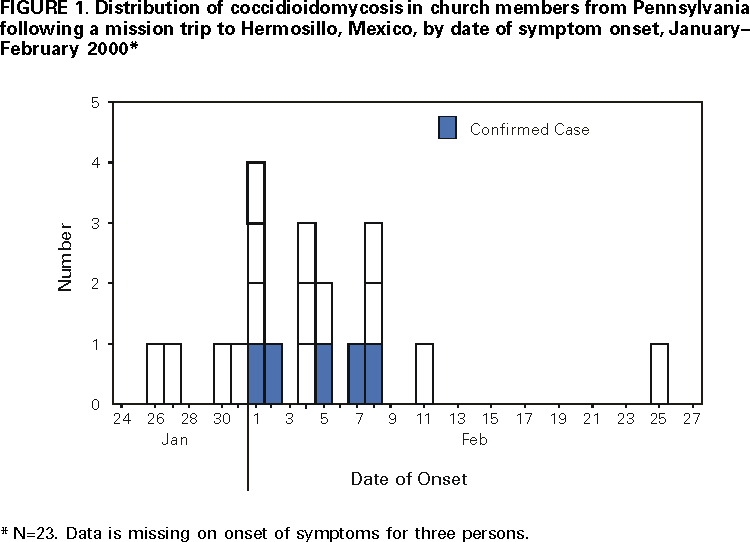 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 11/9/2000 |
|||||||||
This page last reviewed 5/2/01
|