 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hypothermia-Related Deaths --- Suffolk County, New York, January 1999--March 2000, and United States, 1979--1998Hypothermia is the unintentional lowering of core body temperature to <95 F (<35 C) (1). Core body temperature normally is maintained at 97.7 F (36.5 C) (2). Most hypothermia-related deaths occur during the winter in states that have moderate to severe cold temperatures (e.g., Alaska, Illinois, New York, and Pennsylvania) (3). During 1979--1998, New York had the second highest number of hypothermia-related deaths in the United States. This report presents case reports of four hypothermia-related deaths during January 1999--March 2000 in Suffolk County (1999 population: 1,383,847), the largest county in New York excluding New York City, and summarizes hypothermia-related deaths in the United States during 1979--1998. Such deaths can be prevented by educating health-care providers and the public to identify persons at risk for hypothermia. Case ReportsCase 1. On December 15, 1998, an 89-year-old woman with a history of wandering was noticed missing from the adult home facility where she resided and was found shivering in 1 foot of water at the edge of a pond on the property. The temperature that day ranged from 23 F--54 F (--5 C--12.2 C). On admission to a hospital, her rectal temperature was 95 F (35 C). Her medical history included dementia, multiple transient ischemic attacks (TIAs), hypertension, and chronic atrial fibrillation. Her medications included digoxin, furosemide, aspirin, colchicine, and sertraline hydrochloride. On December 21, she developed adult respiratory distress syndrome; she died on January 10, 1999. The death certificate listed the cause of death as complications of environmental exposure with aspiration. Hypertension, arteriosclerotic cardiovascular disease, and dementia were contributory. Case 2. In January 2000, a 51-year-old man wearing a rain-soaked sweater, pants, and work boots was found dead behind a dumpster. On the day he was found, the temperature ranged from 25 F--49 F (--3.9 C--9.4 C); the day before, it had been raining with temperatures in the 50s. Drug paraphernalia was found in his pockets and needle track marks were observed on his arms. According to the police report, the decedent had a history of illegal drug use. Toxicology showed 0.10% ethanol, morphine, codeine, and methadone in his body. The death certificate listed the cause of death as complications of acute and chronic drug abuse and environmental hypothermia. Case 3. In January 2000, a 79-year-old woman who resided in an adult home facility had been missing for 40 minutes. She was found outside, unresponsive, wearing a blouse, sweatshirt, and sweatpants. The temperature that day ranged from 26 F--32 F (--3.3 C--0 C). At a hospital, her rectal temperature was 81 F (27 C). She was treated with hypothermic blankets but died 1 hour later. The decedent had a history of senile dementia, syncope, and TIAs. Her medications included iron sulfate and aspirin. The cause of death was hypothermia with senile dementia and arteriosclerotic cardiovascular disease contributing. Case 4. In March 2000, a 45-year-old homeless man was found dead next to a makeshift bed in a wooded campsite with his shirt partly covered with snow. The temperature that day ranged from 24 F--41 F (--4.4 C--4 C). He was fully clothed, including hat and gloves, and was lying partially in a sleeping bag on top of a canvass pool cover. The decedent had a history of alcohol and drug abuse, but no drugs or alcohol were found in his blood. He had been living in the woods for several years and was last seen several weeks before his death. The death certificate listed the cause of death as probable hypothermia attributed to environmental exposure with chronic alcoholism contributing. New YorkDuring 1979--1998, the age-adjusted death rate for hypothermia was 0.2 per 100,000 population (International Classification of Diseases, Ninth Revision [ICD-9], codes E901.0, E901.8, and E901.9; excludes man-made cold [E901.1])*, compared with the median of 0.4 for the United States. Suffolk County ranked fifth among New York's 62 counties in number of hypothermia-related deaths for persons of all ages. Age-specific death rates in Suffolk County and New York increased with age (Figure 1). Of all hypothermia-related deaths in New York and Suffolk County, 386 (53%; 95% confidence interval [CI]=±3.6%) and 25 (58%; 95% CI=±14.8%), respectively, occurred among persons aged >65 years. In Suffolk County, age-adjusted death rates were three times higher for men than women. United StatesDuring 1979--1998, 13,970 persons died from hypothermia, an average of 699 deaths per year (range: 420--1024 deaths) (Figure 2), and the age-adjusted death rates for hypothermia decreased significantly (p<0.001). Of all hypothermia-related deaths, 6857 (49%; 95% CI=±0.83%) occurred among persons aged >65 years. The age-adjusted rate for hypothermia was approximately 2.5 times higher for men (0.5 per 100,000 population) than women (0.2) during the same period. Reported by: CV Wetli, MD, Office of the Medical Examiner, Dept of Health Svcs, Suffolk County, Hauppauge; P Smith, MD, State Epidemiologist, New York State Dept of Health. Health Studies Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; and an EIS Officer, CDC. Editorial Note:The findings in this report indicate that hypothermia-related deaths in the United States decreased during 1979--1998. In addition, in New York and Suffolk County, hypothermia-related death rates increased by age category and were higher among men, similar to trends observed in the United States. All four case-patients in this report had one or more risk factors for hypothermia-related death (e.g., older age [>65 years], lack of adequate housing, homelessness, mental impairment, drug overdose, and alcohol ingestion) (4). Contributing factors include malnutrition, lack of fitness, severe illness, and drug use or abuse (5). Data in this report are limited by the underreporting of hypothermia in medical records and death certificates (5). Hypothermia-related deaths may be underreported because 1) physical signs of hypothermia may not be recognized; 2) hospitals may not use low-temperature thermometers; 3) medical personnel may be unaware of hypothermia's significance; and 4) an autopsy cannot prove hypothermia as an underlying cause of death (6). In addition, vital record data on hypothermia may not code hypothermia as the underlying cause of death. Mortality estimates are 75%--90% for persons with hypothermia and underlying disease, compared with <10% for those with hypothermia alone (7). Diseases such as hypoglycemia, hypothyroidism, sepsis, and cirrhosis, or drug use (e.g., alcohol, phenothiazines, opiates, clonidine, lithium, barbiturates, and benzodiazepenes) can result in decreased heat production (8). Alcohol use results in central nervous system depression, vasodilation, and blunting behavioral responses to cold. Signs of hypothermia include uncontrollable shivering, confusion, memory loss, drowsiness, exhaustion, fumbling hands, and slurred speech. Severe hypothermia can result in loss of consciousness, apparent apnea, or undetectable pulse. In infants, warning signs of hypothermia include cold, bright red skin and lethargy. Preventive measures include wearing several layers of loosely fitting clothing with a tightly woven, wind-resistant outer layer and wool, silk, or polypropylene inner layers to hold body heat. In cold and windy climates, persons should maintain dry clothing; eat well-balanced meals; drink warm, sweet, nonalcoholic beverages; and avoid exertion because excess perspiration can cause chilling (9). Persons who participate in outdoor recreation should take appropriate precautions, such as wearing wet suits while participating in water-related activities or carrying emergency shelters and heat-generating devices for unexpected weather changes while hiking or camping. During winter months or in areas with low nighttime temperatures, blankets or extra clothing should be kept in vehicles when driving. Measures to prevent hypothermia-related deaths include educating the public and health-care providers (e.g., emergency department, adult home facility, and social services staff) to identify persons at risk and establishing outreach programs that provide warm shelter and adequate clothing. References
* These data were obtained from the Compressed Mortality File (CMF), maintained by CDC's National Center for Health Statistics, and have been prepared in accordance with the external cause-of-death codes from the ICD-9. The CMF contains information from death certificates filed in the 50 states and the District of Columbia. Figure 1 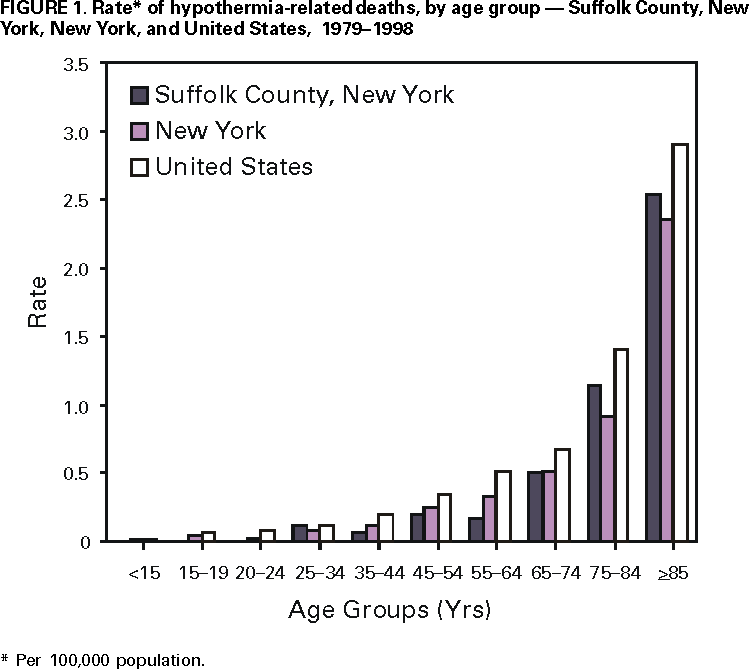 Return to top. Figure 2 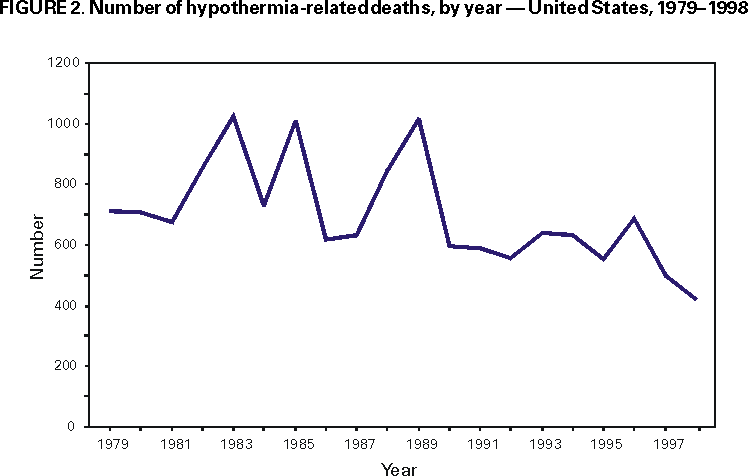 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 2/1/2001 |
|||||||||
This page last reviewed 5/2/01
|