 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Protracted Outbreaks of Cryptosporidiosis Associated With Swimming Pool Use --- Ohio and Nebraska, 2000Swimming is the second most popular exercise in the United States with approximately 400 million pool visits annually (1). During the summer of 2000, five outbreaks of cryptosporidiosis linked to swimming pools were reported to CDC. This report summarizes the investigations of two of these outbreaks involving approximately 1000 cases and provides recommendations to reduce the transmission of pool-related disease. OhioIn July 2000, the Delaware City/County Health Department (DCCHD) learned of several laboratory-confirmed cases of cryptosporidiosis potentially linked to a private swim club. To determine associated exposures, DCCHD, in collaboration with the Ohio State Health Department and CDC, conducted an investigation. A descriptive study and two telephone-based case-control studies were conducted: a community-based study to examine potential sources of the outbreak and a swim club-based study to identify club-related risk factors. Persons were asked about source of drinking water, recent travel, visits to pools and lakes, swimming behaviors, contact with ill persons or young animals, and day care attendance. A clinical case was defined as diarrhea (three loose stools during a 24-hour period) in a person for at least 1 day. A laboratory-confirmed case was defined as diarrhea, vomiting, or abdominal cramps in a person and a stool specimen that tested positive for Cryptosporidium parvum. All case-patients were in central Ohio during June 17--August 18. Case-patients and controls were frequency matched by age. DCCHD identified 700 clinical cases among residents of Delaware County and three neighboring counties. The outbreak began in late June and continued through September (Figure 1). The club closed during July 28--August 4. Of 268 stool samples submitted to DCCHD, 186 (70%) tested positive for Cryptosporidium; 47 laboratory-confirmed case-patients were enrolled in the two case-control studies. The median age of these case-patients was 6 years (range: 1--46 years) and 28 (61%) were female. The median duration of illness was 7 days (range: 1--36 days). Symptoms included diarrhea (91%), loss of appetite (87%), abdominal cramps (83%), and vomiting (35%). Nearly half (45%) reported intermittent diarrhea. Swimming at the private club was strongly associated with illness in the community case-control study. Of the 47 case-patients, 40 (93.6%) went swimming in the pool, compared with 24 (55%) of 44 controls (odds ratio [OR]=42.3; 95% confidence interval [CI]=12.3--144.9). In the club-based case-control study, activities that increased the risk for pool water getting in the mouth (e.g., standing under a pool sprinkler) increased the risk for illness (OR=8.4; 95% CI=1.8--54.8). At least five fecal accidents, one of which was diarrheal, were observed. NebraskaIn August 2000, the Douglas County Health Department, Nebraska, detected an increase in laboratory-reported cases of cryptosporidiosis. Initial cases were linked to a private club with swimming facilities (club A). Additional case-patients reported swimming at club A, at another nearby private club (club B), or at other local pools. The pools at clubs A and B subsequently closed for 2 weeks in mid-August. A case-control study was conducted at club A to identify community and club-specific risk factors. A clinical case was defined as diarrhea (three loose stools during a 24-hour period) in a person who was a member of club A. A laboratory-confirmed case was defined as diarrhea, vomiting, or cramps in a person who had a stool specimen that tested positive for Cryptosporidium. All case-patients were in the Douglas County area during June 3--September 28. Members of club A with laboratory-confirmed or clinical cases of cryptosporidiosis were enrolled in the study. Controls were randomly selected from the club A membership list and frequency matched by age. The outbreak began in mid-June, peaked in mid-August, and tapered off in September, coinciding with the end of the outdoor swimming season in Nebraska (Figure 2). Of 225 clinical and laboratory-confirmed cases, 65 (29%) were laboratory-confirmed and 205 (91%) persons were interviewed. Case-patients were primarily children aged <5 years or adults aged 20--40 years, with a median age of 10 years (range: <1--77 years). Symptoms included diarrhea (94%), abdominal cramps (83%), loss of appetite (74%), nausea (60%), and vomiting (43%). The median duration of diarrhea was 7 days (range: 1--44 days), and nearly half (46%) of patients reported intermittent diarrhea. Thirty-seven case-patients and 36 controls were included in the case-control study at club A. Illness was associated with swimming at club A (OR=5.0; 95% CI=1.48--17.7) and having been splashed with pool water (OR=5.3; 95% CI=1.6--18.9). Swimmers often swam at multiple pool facilities and swim/dive team meets were held at both clubs A and B. Approximately 18% of the case-patients reported swimming while symptomatic, and nearly one third (32%) swam either during illness or during the 2-week period after symptoms subsided. Fecal accidents were observed at both clubs. Reported by: F Veverka, MPH, N Shapiro, MA, Delaware City/County Health Dept, Delaware. MK Parish, MS, S York, MPH, W Becker, DO, F Smith, MD, State Epidemiologist, Ohio Dept of Health. C Allensworth, T Baker, MPH, Douglas County Health Dept, Omaha; P Iwen, MS, Nebraska Public Health Laboratory, T Safranek, MD, State Epidemiologist, Nebraska Dept of Health and Human Svcs. Div of Parasitic Diseases, National Center for Infectious Diseases; Div of Applied Public Health Training, Epidemiology Program Office; Div of Emergency and Environmental Health Svcs, National Center for Environmental Health; and EIS officers, CDC. Editorial Note:Outbreaks of gastrointestinal illness associated with treated recreational water (e.g., swimming pools) appear to have increased in recent years with most being caused by Cryptosporidium (2,3). Although a fecal accident by a swimmer can expose other swimmers to various disease-causing organisms, the probability of transmission of cryptosporidiosis is higher in this setting for two reasons. First, Cryptosporidium oocysts are extremely resistant to chlorine and may remain infective for several days in swimming pool water containing recommended chlorine concentrations (4) and, because of their small size, may not be removed efficiently by conventional pool filters. Second, the high titer of Cryptosporidium in diarrhea from infected persons (5) and the low infectious dose (6) make it possible for a single fecal accident to sufficiently contaminate an entire pool such that accidental ingestion of a few mouthfuls of water can result in infection. The protracted nature of these two outbreaks highlights the challenges faced by health departments and pool managers in detecting and controlling pool-associated cryptosporidiosis outbreaks. The outbreaks went unreported for several weeks, possibly because ill persons often do not seek health care for diarrheal illness (U.S. Department of Agriculture, unpublished data, 1997). During this time, ill persons continued to swim, increasing the likelihood that contamination of the pools continued to occur. It is unclear whether extended pool closure reduced the potential for exposure or contributed to transmission at other pools. A multicomponent approach to outbreak prevention is needed that combines education of swimmers and pool staff, pool design modifications, and improved operations and maintenance procedures. The high incidence of diarrhea in the United States (7) and the continued use of the pools during illness suggest that education of the public is an important component of any prevention strategy. To reduce pool contamination and the spread of cryptosporidiosis and other diarrheal illnesses, public health officials and pool managers should educate staff and patrons about key messages that may reduce recreational water illness transmission. To prevent transmission, persons with diarrhea should not swim, swimmers should avoid swallowing pool water, and persons should practice good hygiene before swimming, after using the restroom, and after changing a diaper. Improved design and management of pools also may reduce the risk for disease transmission. Public health officials and pool operators should consider 1) using separate filtration systems for "kiddie" pools and other pools to decrease the potential for cross-contamination; 2) optimizing filtration rates of kiddie pools without facilitating suction injuries to decrease the length of time that swimmers would be exposed to pathogens; and 3) ensuring that restrooms and diaper changing areas are close to the pool and are clean and adequate in number. Management practices should 1) reinforce that pool operators regularly maintain and monitor pH and free residual chlorine levels to help prevent transmission of most waterborne pathogens; 2) develop policies for pool dis-infection following a fecal accident (8,9); 3) train staff about prevention of recreational water illness transmission; and 4) institute frequent restroom breaks for young swimmers to reduce the potential for fecal accidents. During a pool-associated or other local outbreak of cryptosporidiosis, extra vigilance is necessary to prevent swimming-related disease transmission. Those at risk for serious illness (e.g., immunocompromised persons) should consider not swimming during an outbreak. In addition, because persons ill with cryptosporidiosis often have intermittent diarrhea and Cryptosporidium can be excreted for several weeks after diarrhea subsides (10), ill swimmers should refrain from swimming while ill with diarrhea and should also not swim for a 2-week period after cessation of diarrhea. Operators of implicated pools should intensify education efforts and consider prohibiting diaper- and toddler-aged children from swimming during the outbreak. In addition, health officials should alert pool operators in the geographic area so they can undertake intensive education efforts to prevent infected persons from swimming in and potentially contaminating their pools. Further evaluation is needed to determine the efficacy of extended pool closures on preventing Cryptosporidium transmission. Additional information about prevention of recreational water illness is available at http://www.cdc.gov/healthyswimming. References
Figure 1 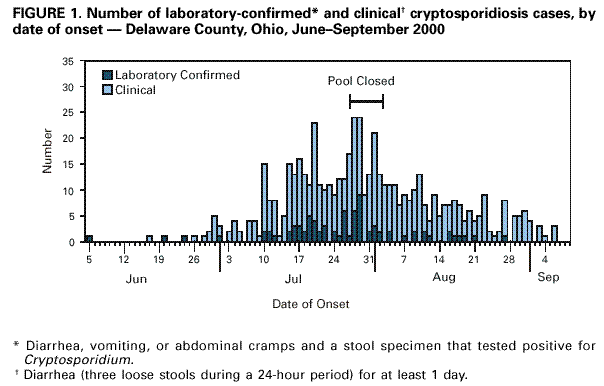 Return to top. Figure 2 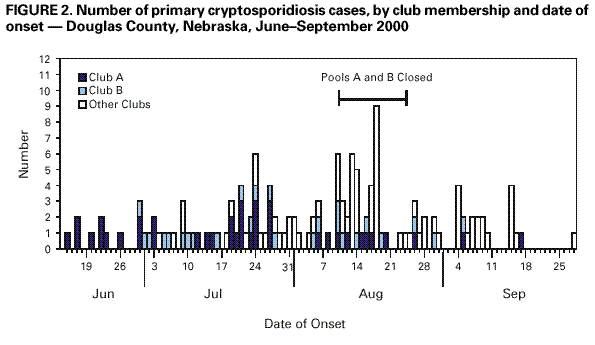 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/8/2001 |
|||||||||
This page last reviewed 6/8/2001
|