 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Racial Disparities in Median Age at Death of Persons With Down Syndrome --- United States, 1968--1997Down syndrome (DS) is the most common identified cause of mental retardation in the United States (1). The prevalence (approximately one in 800 live-born infants) is similar among all racial groups (2). Survival for the first year of life for infants with DS has improved dramatically during the last 50 years, from <50% in a 1942--1952 birth cohort (3) to 91% in a 1980--1996 cohort (4). Most studies of survival in persons with DS have focused on white populations, and little information is available about possible disparities among racial groups. To investigate changes in the age at death among persons with DS by race, CDC analyzed data from multiple-cause mortality files (MCMF) for 1968--1997. This report summarizes the results of the analysis, which indicate that the median age at death of persons with DS increased substantially during this period, but this increase was much greater for whites than for blacks or other races. Identification of the causes for this racial disparity may permit development of strategies to improve the survival of persons with DS, especially those who are black or of other racial groups. MCMF compiled by CDC for 1968--1997 were used to study the median age at death among persons with DS by racial group (5). MCMF include demographic information about the decedent and codes for the underlying cause of death and co-morbid conditions listed on the death certificate. The underlying cause of death and contributing conditions are coded by the states and CDC using the International Classification of Diseases, Adapted for Use in the United States (ICDA-8) or the Manual of the International Statistical Classification of Diseases, Injuries, and Cause of Death, based on the recommendations of the Ninth Revision Conference (ICD-9). From 1968 through 1978, MCMF used ICDA-8 and included up to 14 conditions; from 1979 through 1997, MCMF used ICD-9 and included up to 20 conditions. All deaths that contained the code for DS (ICDA-8 759.3 or ICD-9 758.0) anywhere in the record were selected. Records of persons aged 0 that included the code for pregnancy termination (ICDA-8 773 or ICD-9 779.6) were excluded. The remaining records were defined as "DS-associated deaths." Race was determined from a code in each MCMF record that classified the decedent as either white, black, or races other than white or black. Linear regression was used to test the trend of median age at death by year and estimate ß and its 95% confidence interval (CI). MCMF for 1968--1997 contained records for 33,900 DS-associated deaths. Of these, 64 deaths were excluded because they also were listed as pregnancy terminations. The remaining 33,836 cases represented 56 DS-associated deaths per 100,000 U.S. deaths. The racial distribution among persons with DS was 87.3% white, 11.0% black, and 1.7% other. Among all persons who died in the United States during this period, the racial distribution was 87.0% white, 11.9% black, and 1.1% other. Among all 33,836 DS cases, the median age at death increased from 1 year in 1968 to 49 years in 1997, an average increase of 1.8 (95% CI=1.8--1.9) years per year studied. In comparison, the median age at death in the general population increased from 70 to 76 years or 0.2 (95% CI=0.2--0.3) year per year studied. The median age at death for whites with DS increased from 2 years in 1968 to 50 years in 1997, an average increase of 1.9 (95% CI=1.8--2.0) years per year studied (Figure 1). For blacks during the same period, the median age at death increased from 0 in 1968 to 25 years in 1997, an average increase of 0.7 (95% CI=0.5--1.0) year per year studied. The median age at death for blacks with DS began to improve around 1982. For persons with DS of other racial groups, the median age at death was 0 years in 1968 and 11 years in 1997, representing an average increase of 0.2 (95% CI=0.1--0.3) year per year studied. The median age at death among those with DS of other races began to improve around 1995. The median age at death increased more among persons with DS who were black after 1992 and among those who were of other races after 1995 than it did among whites. Reported by: JM Friedman, PhD, Univ of British Columbia, Vancouver, British Columbia, Canada. National Center on Birth Defects and Developmental Disabilities, CDC. Editorial Note:The increase in the median age at death for persons with DS from 1 to 49 years since 1968 reflects substantially improved survival. However, racial disparity still exists in DS survival, and further study is needed to determine the causes of this disparity. The findings in this report provide little information about the causes for either the improvement or the racial disparity in median age at death. During the study period, treatment of persons with DS changed markedly. In the 1960s, many were institutionalized and relatively few lived with their families after early childhood (6). Today, most children with DS live with their families, and older persons with DS often live in group homes or other facilities in the community (6). Medical care, especially treatment of congenital heart defects among persons with DS, also changed during the study period (7). The findings in this report are subject to at least two limitations. First, the study is based on death certificates (8). The causes of death on death certificates may be incomplete or inaccurate, especially for medical conditions not usually resulting in death and for deaths occurring outside hospitals (9). In particular, DS may not be reported if the certifying physician did not feel that it caused or contributed to death. Incomplete reporting of DS is likely in this study because only approximately half the expected number of DS-associated deaths was observed, assuming a DS prevalence of approximately one in 800 live-born infants (2). The proportion of death certificates that list DS as a diagnosis was similar among whites, blacks, and others, suggesting that the results were not influenced by differences in reporting the diagnosis among persons of different races. Second, this study did not account for the impact of differences and temporal changes in the distributions of age at death within racial groups in the general population. These factors may have contributed to the racial disparity and temporal changes observed. Two factors that might account for the more limited improvement in median age at death of persons with DS who are black or of other races are differences in the frequency of life-threatening malformations and differences in social factors and care provided to persons with DS. No evidence exists that persons with DS who are black or members of other races are more likely to have life-threatening malformations. In this study, the proportion of persons with DS who also had congenital heart defects listed on their death certificates was similar among whites, blacks, and others. Because differences in ascertainment or severity probably do not explain these observations, differences in care received by persons with DS might explain racial disparity in survival. Possibilities include differences in factors that may be associated with improved health in the general population such as socioeconomic status, education, community support, medical or surgical treatment of serious complications, or access to, use of, or quality of preventative health care. A combination of factors seems likely, as appears to be the case for racial disparity in mortality in the U.S. population in general (10). Additional study is needed to determine why persons with DS die much younger if they are black or of other races than if they are white. Identification of these factors may permit development of interventions to eliminate this racial disparity and further improve the survival of all persons with DS. References
Figure 1 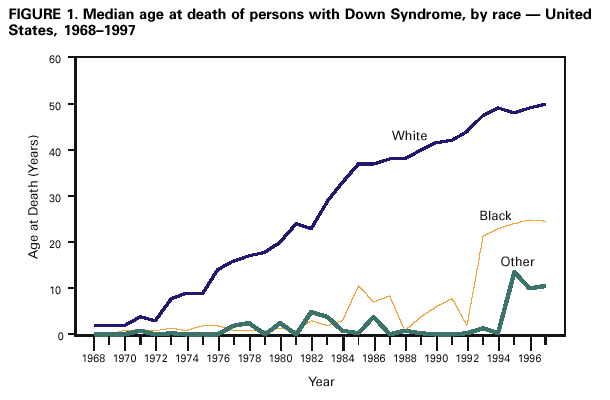 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/8/2001 |
|||||||||
This page last reviewed 6/8/2001
|