 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Hepatitis B Outbreak in a State Correctional Facility, 2000On March 31, 2000, acute hepatitis B was confirmed serologically in a 34-year-old man (index patient) who had been incarcerated for 2.5 years at a high-security state correctional facility and who presented to the facility medical unit with jaundice and abnormal liver enzymes. He reported having unprotected sex with his cellmate as his only risk factor for infection during the 6 months preceding his illness. Serologic testing of the 21-year-old cellmate confirmed that he had chronic hepatitis B virus (HBV) infection. He reported no history of symptoms compatible with hepatitis and was previously unaware of his chronic infection, but he did report having unprotected sex with the index patient and two additional inmates in the dormitory (dorm Y). On May 15, 2000, the state's department of health and department of corrections and CDC initiated an investigation to identify additional cases and determine risk factors for HBV infection. This report summarizes the results of the investigation, which identified additional cases of HBV infection in this correctional facility and underscores the need to implement hepatitis B vaccination in correctional facilities. Current inmates who had resided in dorm Y at any time since October 1, 1999, were offered serologic testing for HBV infection and were interviewed about exposures during the preceding 6 months, including sexual activity, being tattooed, sustaining a cut or injury, being exposed to another inmate's blood, sharing a razor, and injection drug use. Acute HBV infection was defined as the presence of IgM antibody to hepatitis B core antigen (IgM anti-HBc) with or without the presence of hepatitis B surface antigen (HBsAg). Chronic HBV infection was defined as the presence of HBsAg and total (IgG and IgM) anti-HBc, and absence of IgM anti-HBc. Resolved infection was defined as the presence of total anti-HBc, but absence of IgM anti-HBc and HBsAg. Persons testing negative for anti-HBc and HBsAg were considered susceptible to HBV infection. Of 103 eligible inmates, 97 (94%), including the sexual contacts of the inmate with chronic infection, consented to serologic testing. Of these 97 inmates, six (6%) had acute HBV infection, one (1%) had chronic infection, and 16 (16%) had resolved infection. The acute HBV infection rate among susceptible dorm Y inmates was 8%. Two inmates reported nonspecific symptoms (e.g., influenza-like illness) during the preceding 6 months. In addition to the index patient, one of the two other sexual contacts of the inmate with chronic infection had acute infection. The six inmates with acute infection and 70 (95%) of 74 susceptible inmates were interviewed. Having sex with another man was the only risk factor associated with acute HBV infection (risk ratio=12.2; 95% confidence interval=3.5--42.2) and accounted for two of six acute infections (Table 1). The correctional facility is comprised of 14 dormitories housing 96 inmates each; it operates at 99% capacity. Inmates move within the facility to participate in daily scheduled activities and frequently move among dormitories during their incarceration. Condoms are not available to inmates. Because of the HBV transmission in dorm Y, on June 6, 2000, serologic testing was offered to inmates who resided in the remainder of the facility to determine if further HBV transmission had occurred. Of 1247 inmates in the remainder of the facility, 1026 (82%) consented to serologic testing and completed a self-administered questionnaire, which collected information on demographic characteristics and history of behaviors or characteristics that may have placed them at risk for HBV infection both during incarceration and during their lifetime. Of the 1026 inmates, 10 (1%) had chronic HBV infection and 178 (17%) had resolved infection. Of 838 susceptible inmates, five (<1%) were identified with previously undiagnosed acute HBV infection, resulting in an acute infection rate of 0.6% among inmates who did not reside in dorm Y, and an overall infection rate of 1.2% (11 of 918). Of the inmates with acute infection who did not reside in dorm Y, two were housed in one dormitory and the remainder resided in three other dormitories. None reported risk factors for HBV infection during the preceding 6 months. Risk behaviors were evaluated to determine the potential for susceptible inmates to acquire HBV infection. Among the 907 susceptible inmates who completed the questionnaire, 473 (52%) reported at least one exposure while incarcerated that could have resulted in HBV transmission. These included injecting drugs (21 [2%] of 902), having sex with another man (36 [4%] of 899), using a razor that had been used by another inmate (73 [8%] of 900), and receiving a tattoo (429 [48%] of 898). Lifetime histories of risk factors associated with HBV infection also were reported frequently by susceptible inmates and included having received treatment for a sexually transmitted disease (STD) (328 [37%] of 896), having had >50 female sexual partners (110 [13%] of 838), having injected drugs (78 [9%] of 899), and having had sex with men (26 [3%] of 900). To control the outbreak, the state's department of corrections offered hepatitis B vaccination to all susceptible inmates in dorm Y. In addition, acutely and chronically infected inmates were notified of their infection status, received a clinical assessment, and postexposure prophylaxis was provided to their contacts. The state's department of health and department of corrections are collaborating to implement routine hepatitis B vaccination for all inmates in the correctional system. Reported by: State Dept of Health; State Dept of Corrections. Epidemiology Program Office; Div of Viral Hepatitis, National Center for Infectious Diseases; Div of STD Prevention, National Center for HIV, STD, and TB Prevention; and an EIS Officer, CDC. Editorial Note:The findings in this report document HBV transmission in a correctional facility, including a cluster of cases of acute infection in one dormitory and additional cases distributed throughout the facility. Most persons with acute HBV infection in the correctional facility were asymptomatic, and serologic surveys were needed to determine the extent of HBV transmission. The overall infection rate of 1% reflected infections acquired during the preceding 6 months and was higher than the estimated incidence of 1% per year in previous studies (1,2). This serologic survey also indicated that 1% of inmates had chronic infection and that none were aware of their infection status. HBV is transmitted primarily by percutaneous or permucosal exposures to an infected person. Risk factors associated with HBV infection include having multiple sex partners, having had an STD, being a man who has sex with men, injection drug use, and being a sexual or nonsexual household contact of a person with chronic HBV infection (3). Receiving a tattoo has not been associated with community acquired HBV infections among nonincarcerated populations in the United States (4); however, transmission could occur if the tattoo is applied using contaminated equipment. Sex with another man accounted for only 20% of new infections in this investigation. However, this and other behaviors prohibited by the correctional facility (e.g., injecting drugs) probably are underreported by inmates. Inmates with previously unrecognized chronic HBV infection may have served as a source for infection, similar to household contacts of persons with chronic infection (5). Housing data were not available to determine if persons with acute HBV infection were more likely to have been a cellmate of a chronically infected inmate. The findings in this report are consistent with previous reports of HBV transmission in prison settings (1,2). Since 1982, the Advisory Committee on Immunization Practices has recommended hepatitis B vaccination of long-term inmates with a history of risk factors for infection (3). Although a large proportion of inmates in this prison reported current or previous risk factors for HBV infection, none of the susceptible inmates had been vaccinated. In the state correctional system in this report, approximately one third of inmates are released each year (Department of Corrections, unpublished data, 2000). Previously incarcerated persons represent a population at risk for HBV infection. Approximately 30% of persons with acute hepatitis B report a history of incarceration (6). Hepatitis B vaccination of prisoners would prevent ongoing HBV transmission among inmates in prison facilities and after they have been released into the community. Because of the high proportion of inmates with previous risk factors for HBV infection and the difficulty in ascertaining current risk factors, experts in correctional health recommend vaccination of all inmates (7). Some states have implemented successfully routine hepatitis B vaccination of prisoners. However, identifying resources to purchase and administer vaccine remains the major barrier to national implementation of this strategy. Partnerships between state health and corrections departments can help to implement hepatitis B vaccination and promote effective strategies for prevention of other STDs and infections in correctional facilities (8). References
Table 1 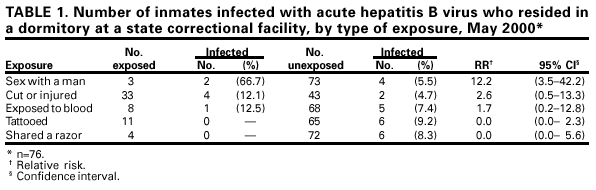 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 7/2/2001 |
|||||||||
This page last reviewed 7/2/2001
|