|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
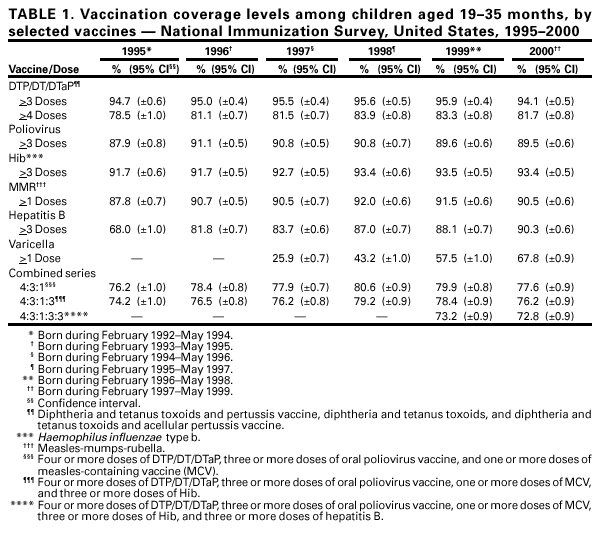
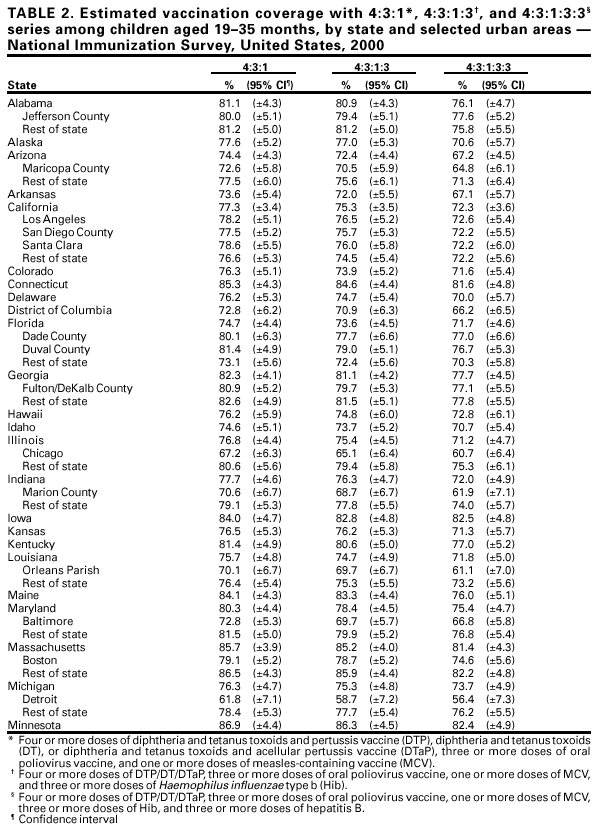
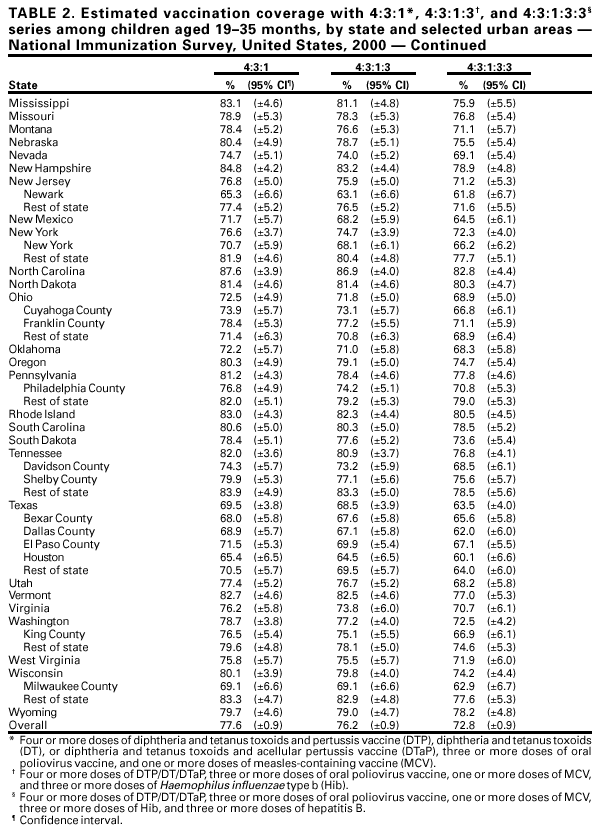
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. National, State, and Urban Area Vaccination Coverage Levels Among Children Aged 19--35 Months --- United States, 2000Since the early 1970s, childhood vaccination has prevented millions of illnesses and tens of thousands of deaths (1). For these health benefits to continue, high levels of vaccination coverage must be attained for each new birth cohort and must be monitored to ensure protection from disease, to characterize undervaccinated populations, and to evaluate efforts to increase coverage. The National Immunization Survey (NIS) provides ongoing national estimates of vaccination coverage among preschool-aged children for the 50 states and 28 selected urban areas* (2,3). For this report, NIS data collected during 2000 were compared with 1999 data; findings indicate that, during 2000†, significant increases were reported on the national level of vaccination coverage with varicella and hepatitis B, and small but statistically significant decreases were reported in coverage with diphtheria, and tetanus toxoid, and pertussis vaccine. Coverage with poliovirus vaccine, Haemophilus influenzae type b vaccine, and measles-mumps-rubella vaccine were not significantly different from 1999. As in previous years (4), coverage varied among states. To maximize coverage among preschool-aged children, vaccination providers should continue to apply such strategies as reminders and recalls. To collect vaccination data for children aged 19--35 months, NIS uses a random-digit--dialing sample of telephone numbers for each survey area. During 2000, 34,087 household interviews were completed. Contacted providers submitted data for 22,958 children; the data then were weighted to represent all children surveyed and to account for nonresponding households, lower vaccination coverage among children in households without telephones, and changes in natality patterns. During 2000, national vaccination coverage with three doses of any diphtheria and tetanus toxoids and pertussis vaccine (DTaP3) declined from 95.9% in 1999 to 94.1%; coverage with four doses of any diphtheria and tetanus toxoids and pertussis vaccine (DTaP4) declined from 83.3% in 1999 to 81.7%. Coverage was not significantly different from 1999 to 2000 for three doses of oral poliovirus vaccine (OPV3) (from 89.6% to 89.5%), three doses of Haemophilus influenzae type b vaccine (Hib3) (from 93.5% to 93.4%), and one dose of measles-mumps-rubella vaccine (1MMR) (from 91.5% to 90.5%) (Table 1). During 2000, coverage with one dose of varicella vaccine increased from 57.5% in 1999 to 67.8%, and coverage with three doses of hepatitis B vaccine (HepB3) increased from 88.1% in 1999 to 90.3%. National coverage with combined vaccination series 4:3:1:3 (DTaP4, OPV3, one dose of measles-containing vaccine, and Hib3) and 4:3:1:3:3 (4:3:1:3 series and HepB3) decreased from 1999 to 2000 (78.4% to 76.2% and 73.2% to 72.8%, respectively). State-specific and urban-area coverage varied§ (Table 2). Reported by: Data Management Div, National Immunization Program, CDC. Editorial Note:National coverage with routinely recommended childhood vaccines increased substantially after the Childhood Immunization Initiative was implemented in 1993 (5). Although coverage with recommended vaccines for each new birth cohort remains high, vigilance is needed to maintain these levels. The slight declines in coverage with certain vaccines from 1999 to 2000 do not pose a major public health risk; however, should vaccine-preventable diseases be introduced into low coverage geographic areas, the accumulation of susceptible persons might serve as a reservoir to disseminate diseases. Reduced vaccination coverage may be the result of missed opportunities to vaccinate and incomplete or scattered vaccination records (6,7). Some states and counties have compiled population-based, computerized registries that contain vaccination information on nearly all preschool-aged children. These registries enable providers to identify children who are due for vaccinations and to automatically review a child's vaccination history to determine the vaccines needed on a particular visit. The findings in this report are subject to at least three limitations. First, NIS is a telephone survey; although statistical adjustments compensate for nonresponse and nontelephone households, and other potential sources of bias, some bias might remain. Second, NIS relies on provider-verified vaccination histories. The completeness of provider records and data provided to NIS is unknown. Third, because of sampling uncertainly in NIS, particularly on the subnational level, results should be interpreted with caution. Standards for pediatric vaccination practices that first were recommended in 1992 by the National Vaccine Advisory Committee (8) and were endorsed by medical professional organizations are being revised to reflect a largely privatized vaccination delivery system with improved public financing for vulnerable children through the Vaccines for Children program and an emphasis on adolescent vaccination. State and local vaccination programs and public and private vaccination providers should continue to use reminders and recalls, vaccinate at every opportunity, and administer multiple vaccinations when indicated to ensure the highest possible coverage among preschool-aged children. References¶
*Jefferson County, Alabama; Maricopa County, Arizona; Los Angeles, San Diego County, and Santa Clara, California; District of Columbia (DC); Dade and Duval counties, Florida; Fulton/DeKalb County, Georgia; Chicago, Illinois; Marion County, Indiana; Orleans Parish, Louisiana; Baltimore, Maryland; Boston, Massachusetts; Detroit, Michigan; Newark, New Jersey; New York, New York; Cuyahoga and Franklin counties, Ohio; Philadelphia County, Pennsylvania; Davidson and Shelby counties, Tennessee; Bexar, Dallas, and El Paso counties, and Houston, Texas; King County, Washington; and Milwaukee County, Wisconsin. † For this reporting period (January--December 2000), NIS included children born during February 1997--May 1999. § Range of state-specific coverage during 2000---4:3:1:3 combination: 68.2%--86.9%; 4:3:1:3:3 combination: 63.5%--82.8%. DTaP3: >90%; DTaP4: 72.8%--91.6%. OPV3, 1MMR, and HepB3: >85% except in a few states. Hib3: >90% except in three states. Variation in coverage was greatest among children who had received one dose of varicella vaccine: 38.0%--84.5% (estimate). ¶ All MMWR references are available on the Internet at <http://www.cdc.gov/mmwr>. Use the search function to find specific articles.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/3/2001 |
|||||||||
This page last reviewed 8/3/2001
|