 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Healthy Lifestyle Characteristics --- Michigan, 1998 and 2000Most persons with chronic diseases such as cardiovascular disease, cancer, diabetes, and chronic lung disease share multiple common risk factors and lifestyle behaviors (1). Tobacco use, poor diet, and physical inactivity have been identified as the leading contributors to overall mortality in the United States, accounting for one third of all deaths (2); Michigan has a particularly high burden of chronic disease-related mortality (3). To characterize the prevalence of four healthy lifestyle characteristics (HLCs) (i.e., healthy weight, adequate fruit and vegetable consumption, regular leisure-time physical activity [LTPA], and not smoking) in Michigan residents, data were analyzed from Michigan's Behavioral Risk Factor Surveillance System (BRFSS) for 1998 and 2000. This report summarizes the results of the analysis, which indicate that the proportion of Michigan residents who engaged in all four healthy lifestyle practices was extremely low, and that the prevalence was influenced by sex, education and self-reported health status. The comprehensive assessment of HLCs may be a useful adjunct to chronic disease surveillance. BRFSS is a random-digit--dialed telephone survey of the noninstitutionalized U.S. population aged >18 years. Data were analyzed from 4816 adults for 1998 and 2000 combined. Missing data from 502 persons resulted in a sample size of 4314. Healthy weight was defined as having a body mass index between 18.5 and 25.0. Adequate fruit and vegetable consumption was defined as eating five or more fruits and vegetables daily. Regular LTPA was defined as at least 30 minutes of physical activity five or more times per week. Not smoking was defined according to self-reported absence of current cigarette use (i.e., former or never versus current). Data were weighted to adjust for the probability of selection and the distribution of the state's population by age, race/ethnicity, and sex. Descriptive analyses, including age-adjusted prevalence estimates, were generated for each demographic variable (age, race/ethnicity, education, and household income) and self-reported health status using SUDAAN. Data were standardized by age to the projected 2000 U.S. population. Significant differences in the adjusted odds ratios (AORs) for engaging in all four HLCs were identified using a multiple logistic regression model that contained all independent variables. An estimated 37.9% (95% confidence interval [CI]=36.3%--39.5%) of Michigan adults had a healthy body weight, 22.8% (95% CI=21.4%--24.2%) ate the recommended amount of fruits and vegetables, 25.9% (95% CI=24.4%--27.4%) engaged in regular LTPA, and 72.3% (95% CI=70.8%--73.8%) did not smoke. Overall, 11.2% (95% CI=10.1%--12.3%) of adults engaged in none of these practices, 38.6% (95% CI=37.0%--40.2%) in one, 33.3% (95% CI=31.7%--34.9%) in two, 13.9 % (95% CI=12.8%--15.0%) in three, and 3.0% (95% CI=2.5%--3.5%) in all four. The prevalence of engaging in all four HLCs was significantly different by sex, education, and health status (p<0.05) (Table 1). The prevalence of engaging in all four HLCs was lower in men (age-adjusted prevalence=1.6%) than in women (age-adjusted prevalence=4.5%; AOR=0.3; 95% CI=0.2--0.5). The prevalence of engaging in all four HLCs increased with education. The prevalence in college graduates was more than three times higher than in those with a high school education or less (AOR=3.2; 95% CI=1.7--6.1). However, the age-adjusted prevalences were still very low in all three education groups (Table 1). The prevalence of engaging in all four HLCs decreased with decreasing health status. Persons reporting excellent health had a much higher age-adjusted prevalence (7.1% [95% CI=5.3%--8.9%]) than adults with fair or poor health (1.0% [95% CI=0.1%--1.9%; AOR=0.1; 95% CI=0.04--0.4]). However, the prevalence rates in all four groups were low (Table 1). Reported by: MJ Reeves, PhD, Dept of Epidemiology, College of Human Medicine, Michigan State Univ, East Lansing; A Rafferty, PhD, H McGee, MPH, C Miller, PhD, Bur of Epidemiology, Michigan Dept of Community Health. Cardiovascular Health Br, Div of Adult and Community Health, and Physical Activity and Health Br, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report document the low prevalence of healthy lifestyles in Michigan. The prevalence of HLCs in this report is consistent with that in the Nurses Health Study for a similar grouping of five healthy lifestyle behaviors (4) and is indentical to that from the overall 2000 BRFSS data. When compared with other states, obesity and smoking in Michigan are higher than the national average (5). However, the daily consumption of five fruits and vegetables in Michigan is consistent with the national average, and Michigan ranked among the top 10 states for participation in regular and sustained physical activity in 2000. Disease risk, especially that related to cardiovascular disease, has usually been examined separately. Some studies have measured disease risk more comprehensively by combining factors such as smoking, obesity, hypertension, and high blood cholesterol (6). This study used a similar approach by assessing the combination of healthy factors that reduce disease risk, which may be a useful adjunct to the more traditional risk factor surveillance method. The findings in this report are subject to five limitations. First, data were self-reported and some responses may be considered socially undesirable. As a result, respondents may both underreport weight (7) and overreport LTPA or fruit and vegetable consumption. Second, BRFSS collects information about LTPA only and may underestimate total activity. Third, BRFSS estimates of daily fruit and vegetable consumption are similar to estimates based on multiple records but are smaller than estimates based on more extensive food-frequency questionnaires (8). Fourth, the number of black respondents in this study was too small for meaningful analysis. Finally, noncoverage and nonresponse biases related to telephone survey data may affect estimates. Findings from previous epidemiologic studies (6,9) underscore the need for comprehensive primary prevention activities to reduce the prevalence of common chronic disease risk factors. Primary prevention may be a useful strategy in promoting the adoption and maintenance of HLCs (10). Primary prevention includes addressing the underlying social determinants that lead to behavioral and physiologic risk factors by mobilizing both health-care providers and the general population to adopt new policies. These policies include regulatory, educational, and environmental changes designed to facilitate the implementation of prevention programs. In Michigan, two initiatives sponsored by the Michigan Department of Community Health (MDCH) and the Governor's Council on Physical Fitness promote physical activity and healthy weight. First, a voluntary Exemplary Physical Education Curriculum provides school-aged children with the fitness levels, motor skills, activity-related knowledge, and personal/social skills needed for an active life. Second, environmental changes that make it easier and safer for persons to be physically active are encouraged through the "Promoting Active Communities Award," which recognizes communities that enact policies to promote physical activity. To promote a healthy diet, MDCH's 5-A-Day program provides technical support, information, and materials to local agencies to assist them in conducting local programs. MDCH also works with grocery stores to provide education materials and grocery rewards to consumers to encourage them to eat fruits and vegetables. References
Table 1 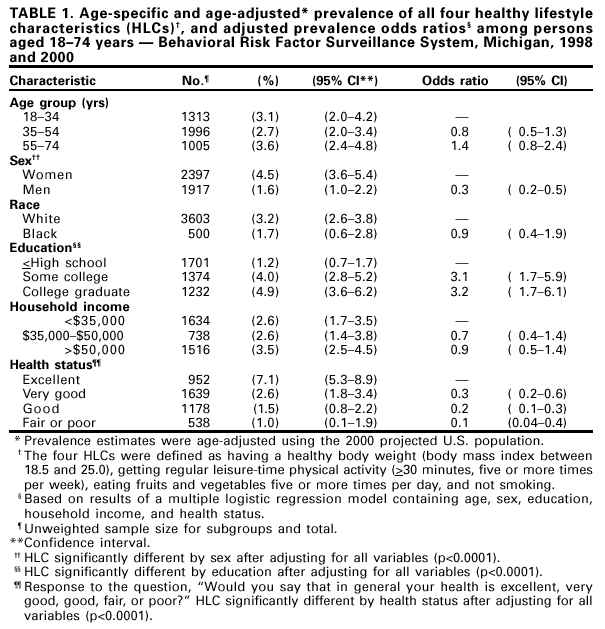 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/7/2001 |
|||||||||
This page last reviewed 9/7/2001
|