 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Shigellosis Outbreak Associated With an Unchlorinated Fill-and-Drain Wading Pool --- Iowa, 2001On June 15, 2001, local physicians reported 11 cases of diarrhea to a county health department. Stool samples from two of these persons were culture confirmed as Shigella sonnei; one person was hospitalized. A preliminary investigation found that nine of these persons recently had visited a large city park with a wading pool. The Iowa Department of Public Health was asked to assist in an investigation of this outbreak. This report summarizes the results of the investigation, which implicated the inadequately disinfected wading pool as the source of the outbreak and presents strategies for preventing such outbreaks. Beginning on June 15, telephone interviews were conducted using a questionnaire that included information about demographics, illness history, participation in group gatherings, water activities, and use of the park or wading pool. Ill persons were asked to identify others who were at the park or had similar symptoms. A primary case was defined as self-reported diarrhea in a person within 72 hours of visiting the park during June 11--13. A secondary case was defined as self-reported diarrhea in a person within 72 hours of household contact with a primary case-patient. Of 89 persons interviewed, 69 met one of the case definitions. Of these, 45 (65%) were categorized as primary cases and 24 (35%) as secondary cases. Stool samples from 16 primary case-patients and 10 secondary case-patients were laboratory confirmed as S. sonnei, and all 26 isolates were indistinguishable by pulse field gel electrophoresis (PFGE). Of 24 isolates tested at a clinical laboratory, 16 (67%) were resistant to ampicillin and sensitive to trimethoprim-sulfamethoxazole, cefotaxime, and levofloxacin. Illness onset among primary case-patients occurred during June 12--14 (Figure 1). The median age was 6 years (range: 1--31 years); 23 (51%) were female. Symptoms included diarrhea (100%), nausea (51%), vomiting (47%), bloody diarrhea (39%), and headache (29%). Seven (16%) patients were hospitalized. Pool exposure was associated significantly with illness (risk ratio=5.7; 95% confidence interval=1.6--20.4). Illness onset among the 24 secondary case-patients occurred during June 15--22 (Figure 1). The median age was 24 years (range: 0--63 years); 14 (58%) were female. The pool, which has been in operation for approximately 60 years, is 40 feet in diameter, has a maximum depth of 14 inches, and has a 9400-gallon capacity. It is frequented by diaper- and toddler-aged children and as many as 20--30 children may be in the pool at one time. The pool is a "fill and drain" system and is filled each morning with potable city water through a direct inlet pipe and a centrally located fountain; it is drained and left empty each evening. The pool includes a backflow device but has no recirculation or disinfection system (i.e., pump, filter, or mechanical disinfection system). Each morning before filling, the pool is rinsed with a high-pressure washer and is scrubbed with a chlorine cleanser twice weekly. However, chlorine levels were not monitored and chlorine was not added to the pool water. Samples from the pool and other water sources in the park, including drinking fountains and faucets, were collected on June 15 and tested by the Colilert test, a rapid procedure to determine the presence of fecal coliforms. One pool sample tested positive for fecal coliforms and Escherichia coli. The pool was closed on June 15. Reported by: CJ Lohff, MD, GM Nissen, ML Magnant, MP Quinlisk, MD, State Epidemiologist, Iowa Dept of Public Health; CL Tieskoetter, PL Kowalski, Visiting Nurse Association of Dubuque; PA Buss, PhD, Dubuque County Health Dept; TA Link, MR Corrigan, City of Dubuque Health Svcs Dept; JP Viner, MD, Dubuque County Board of Health; AJ Behnke, United Clinical Laboratories, Dubuque; MS DeMartino, AK Houston, Univ of Iowa Hygienic Laboratory, Iowa City, Iowa. Div of Bacterial and Mycotic Diseases and Div of Parasitic Diseases, National Center for Infectious Diseases, CDC. Editorial Note:In this outbreak, the drain-and-fill pool contained municipal water (0.4--0.5 ppm free available chlorine) with no subsequent chlorination so that the pool was probably unchlorinated for most of the time it was in use. Inadequate disinfection of this pool, combined with heavy use by diaper- and toddler-aged children, who are often incontinent and may have an increased prevalence of enteric infections, created a favorable environment for transmission of shigellosis. Transmission of shigellosis over several days may have been a result of the residual contaminated water left in the pipes after draining the pool and persons with diarrhea visiting the pool on subsequent days. The infectious dose for Shigella (1) is low; as a result, a small volume of ingested water can cause infection. The lack of chlorination that led to transmission of shigellosis in this wading pool also increased the risk for spreading life-threatening pathogens such as E. coli O157:H7. This outbreak together with surveillance data that suggest an increase in disease outbreaks associated with recreational water exposure (2) illustrate the need for strict adherence of recreational water venues to existing health codes, enforcement of these codes, and education of pool operators about adequate disinfection and maintenance of pool water quality. Improved facility design and adequate water treatment can decrease the risk for transmission of illness. In addition to improved pool design and improved management and maintenance, increased education of pool staff and the public about the potential for spreading recreational water illness and development of strategies for reducing the spread of swimming-related illness is crucial to decreasing transmission (3). Swimming is a shared water activity that can result in disease transmission, even with adequate chlorination, when water becomes contaminated and is subsequently swallowed. Strategies for prevention include 1) not swimming when ill with diarrhea, 2) not swallowing recreational water, and 3) practicing good hygiene when using a pool. Parents should take children on bathroom breaks regularly, use appropriate diaper changing areas, wash hands after using the toilet or changing diapers, and shower before entering the pool. Swim pants and diapers do not prevent leakage of diarrhea; therefore, they are not an acceptable solution for a child with diarrhea and are not a substitute for frequent diaper changing. Approximately 10,000 cases of S. sonnei are diagnosed each year in the United States, and most occur in young children (4). Subsequent to the outbreak described in this report, a communitywide outbreak of shigellosis involving several local day care centers occurred; PFGE patterns were identical for both swimming-related and community-outbreak isolates. The ease with which single outbreaks can expand into communitywide outbreaks of S. sonnei (5) underscores the importance of educating the community about potential modes of transmission (e.g., child care facilities, food handlers, and swimming) and the implementation of appropriate prevention recommendations during outbreaks (e.g., thorough hand washing after using restrooms, changing diapers, and before handling/preparing food, enforcement of exclusion criteria at child care facilities, and exclusion of persons from swimming while ill with diarrhea). Child care facilities should follow strict hygiene recommendations, including supervised hand washing for young children, and may consider refraining from using water play tables and inflatable pools that may lead to transmission. In addition, communication with pool operators about ongoing outbreaks may improve vigilance in maintaining disinfectant levels necessary to reduce the risk for transmission among bathers at community pools. Additional information about preventing recreational water illness is available at <http://www.healthyswimming.org> (3). References
Figure 1 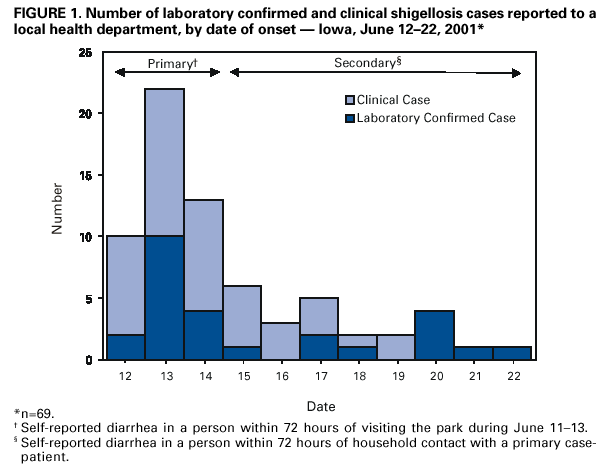 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 9/21/2001 |
|||||||||
This page last reviewed 9/21/2001
|