|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
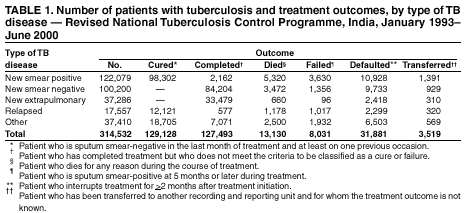
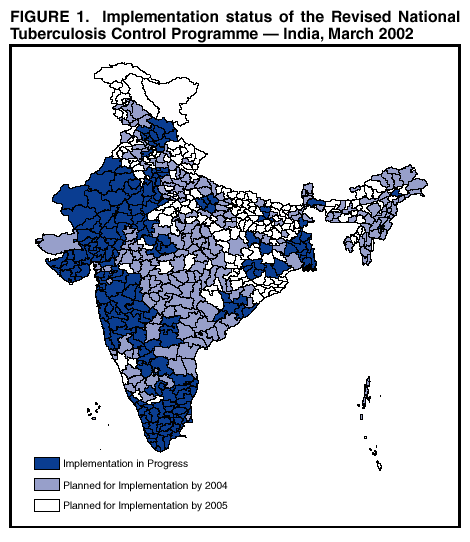
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Tuberculosis Control --- India, 2001Every year, approximately 2 million persons in India develop tuberculosis (TB), accounting for one fourth of the world's new TB cases (1). Organized TB control activities have existed in India for 40 years; however, the quality of diagnosis and treatment of TB in the public and private sectors has been variable, and TB incidence and prevalence trends have not changed substantially over this time (2). In 1992, the Indian government established a Revised National Tuberculosis Control Programme (RNTCP) using the directly observed treatment, short-course (DOTS) strategy recommended by the World Health Organization (WHO) (3). The DOTS strategy consists of sustained government commitment, effective laboratory-based diagnosis, standard treatment given under direct observation, secure drug supply, and systematic monitoring and evaluation. RNTCP was implemented in pilot areas beginning in 1993; large-scale implementation of the program began in late 1998. This report summarizes the process, outcomes, and challenges of RNTCP in India. RNTCP has implemented DOTS rapidly and has yielded positive results in TB control; however, continued commitment from Indian government authorities and the international community is needed to sustain and expand this ongoing program. During 1993--2001, under RNTCP, patients diagnosed in health-care facilities with cough lasting >3 weeks underwent three sputum smear examinations over a 2-day period. If all three acid-fast bacilli (AFB) smears were negative, 1--2 weeks of broad-spectrum antibiotics were prescribed. If some but not all of the specimens were positive, or if a patient with negative smears continued to have symptoms after 1--2 weeks of broad-spectrum antibiotics, a chest radiograph was taken, and if indicative of disease, the patient was treated for TB. All TB treatment was given three times weekly on alternate days; the diagnostic evaluation and the entire course of treatment were free of charge. During the first 2 months of treatment (intensive phase), patients were treated with isoniazid, rifampin, pyrazinamide, and ethambutol (streptomycin was added for retreatment patients, and ethambutol was omitted for smear-negative, nonseriously ill patients); every dose was observed directly by either a health-care provider or a nonfamily community member. For the remaining 4--6 months of treatment (continuation phase), either isoniazid and rifampin or isonizaid, rifampin, and ethambutol were prepared into weekly packs, and at least the first dose each week was observed directly. To prevent drug shortages during TB therapy, medications for both phases of treatment were maintained in individualized patient boxes containing the entire course of treatment for a given patient at the health facility or residence of the community volunteer providing DOTS. Recording and reporting of case detection and treatment outcomes were conducted according to WHO recommendations (3). As of November 2001, RNTCP offered TB control services to regions comprising >40% of the country's population (>440 million persons), compared with <2% in mid-1998 (Figure 1). To prepare for service delivery under RNTCP, since 1998, approximately 3,000 small laboratories have been upgraded for smear microscopy, 2,000 contractual staff hired, approximately 200,000 health-care workers trained in different aspects of DOTS service provision, and approximately 500 million tablets of anti-TB medication distributed. During 2001, approximately 300,000 adult outpatient visits were recorded per day in facilities covered by RNTCP, with approximately 5,000 patients examined for TB and approximately 1,300 patients started on treatment each day of operation. Indicators of the quality of case-detection activities include the proportion of patients with newly diagnosed pulmonary TB who are sputum smear-positive for AFB (which should be >50% in a well-functioning program) (3). During April--June 2001, 179 (95%) of 189 districts reported that >50% of all new pulmonary TB patients were diagnosed as sputum smear-positive for AFB, indicating high diagnostic quality in these districts. One year following the start of treatment, 256,621 (80%) patients had been treated successfully, and 98,302 (81%) patients who were initially sputum smear-positive had laboratory evidence of sputum conversion to negative (Table 1). During April--June 2000, 77 (75%) districts had treatment success rates* of >80%. However, previously treated patients had outcomes that were slightly less favorable than new TB patients (71% versus 83% treatment success). Patients who had previously failed treatment (those who were sputum smear-positive at 5 months or later during an earlier course of treatment) had a significantly higher risk for remaining smear-positive when treated again than did other types of retreatment patients, such as successfully treated patients that relapsed or those who prematurely discontinued treatment (12.9% versus 5.8% and 5.2% respectively, p<0.001). Reported by: GR Khatri, MD, Ministry of Health and Family Welfare; TR Frieden, MD, Stop Tuberculosis Unit, World Health Organization, Regional Office for South East Asia; India Country Office, World Health Organization, New Delhi, India. CR Wells, MD, Div of Tuberculosis Elimination, National Centers for HIV, STD and TB Prevention; L Thorpe, PhD, EIS Officer, CDC. Editorial Note:Despite the availability of highly effective and inexpensive drugs, TB causes more deaths per year in India (421,000) than malaria, hepatitis, meningitis, nutritional deficiencies, sexually transmitted diseases, leprosy, and tropical diseases (e.g., dengue fever, trypanosomiasis, schistosomiasis, leishmaniasis, lymphatic filariasis, and onchocerciasis) combined (258,000) (4). Since 1993, India has implemented successfully a TB control program using the WHO-recommended DOTS strategy. Many of the principles for diagnosis and treatment of the DOTS strategy were derived from studies conducted in India that demonstrated the effectiveness of ambulatory treatment of TB, the necessity and feasibility of DOTS, the efficacy of intermittent treatment with anti-TB drugs (twice weekly rather than daily), and the feasibility of case detection through sputum smear microscopy in primary-care settings (5). However, only recently have these findings been applied widely to establish TB control in large areas of India. The 4% death rate recorded in RNTCP areas since implementation is substantially lower than previously documented death rates of up to 29% among treated smear-positive TB patients in non-RNTCP areas (6). Several obstacles impede the expansion of TB control under RNTCP (7). First, diagnosis and treatment of TB are uncoordinated and inconsistent because many patients initially receive TB care through the large private health-care sector, pharmacies often sell anti-TB drugs over the counter, and TB notification requirements are not enforced routinely. Second, poverty impedes program performance. Many areas lack regular electric supply, limiting the effectiveness of binocular microscopy. Economic hardships and drought cause large-scale migration, reducing treatment completion and cure rates. Third, a patient-centered approach to care---one that actively helps patients by providing them with transportation to health facilities, food, and social support to overcome obstacles to completion of treatment---is not practiced widely in India. Fourth, anti-TB drug resistance, which reflects current or past poor program performance, is difficult to treat and might account for the noticeably higher treatment failure rate among retreated TB patients. In several surveyed areas of India, 1.0%--3.3% of new TB patients have multidrug-resistant TB (MDR-TB), which is resistant to at least isoniazid and rifampin, the two most effective anti-TB drugs (8). This is higher than in many countries, but much lower than in some high-prevalence areas (e.g., areas in the former Soviet Union [10%--15%] and New York City in the early 1990s [7%]) (8). However, even if as few as 2% of new patients were to have MDR-TB, this would represent an estimated 20,000 new infectious cases of MDR-TB in India every year. In areas with relatively good performance, pilot projects of expanded programs to treat MDR-TB should be considered. Finally, although this report does not assess the level of human immunodeficiency virus (HIV) infection among TB patients, the increasing prevalence of HIV in India represents a serious threat to TB control efforts. Approximately 4 million persons in India (<1% of the population) are infected with HIV, of which approximately half also are infected with M. tuberculosis (9). An additional 140,000 TB cases have been estimated annually among tuberculin skin test-positive HIV-infected persons (9). The TB control program in India, already one of the largest public health programs in the world, continues to expand, with plans to cover 80% of the country by 2004 and 100% by 2005. The implementation of RNTCP has resulted in a net savings of more than $400 million in economic costs; effective nationwide implementation by 2005 would save more than $27 billion through 2020 (10). Sustaining and expanding this program will require continued high-level commitment from the central and state governments of India, supplemented by continued and coordinated assistance from international and bilateral organizations. Progress toward TB control in India is critical to global TB control and has direct implications for TB elimination efforts in the United States because nearly half of all TB cases in the United States occur among foreign-born persons, a substantial proportion of whom (nearly 10%) are immigrants from India (10). With immigration from India to the United States rising, India's proportionate contribution to U.S. domestic TB will probably increase. References
* The sum of smear-positive patients who have laboratory evidence of sputum conversion to negative (cure) and those who have completed treatment without final laboratory confirmation of cure.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 3/21/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 3/21/2002