|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
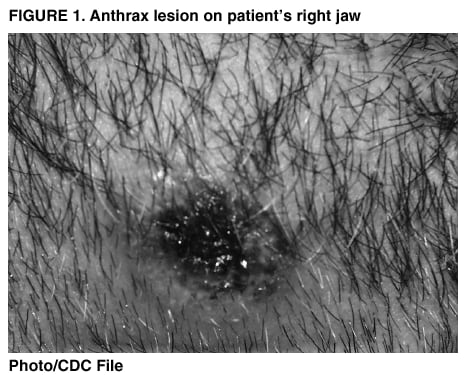
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Suspected Cutaneous Anthrax in a Laboratory Worker --- Texas, 2002On March 6, 2002, CDC's National Institute for Occupational Safety and Health (NIOSH) received a request for a health hazard evaluation from the director of Laboratory A to assist in the evaluation of a worker who had been diagnosed with cutaneous anthrax. Laboratory A, a provisionally approved Laboratory Response Network level B laboratory, had been processing environmental samples for Bacillus anthracis in support of CDC investigations of the bioterrorist attacks in the United States during fall 2001. Since March 7, CDC has interviewed the ill laboratory worker and other workers at the laboratory and conducted environmental assessments of the workplace. This report summarizes the epidemiologic and environmental investigation of this case, which indicates that the likely source of exposure was the surface of vials containing B. anthracis isolates that the worker placed in a freezer on March 1. Laboratory workers handling specimens of B. anthracis should follow recommended procedures to minimize the risk of B. anthracis transmission and anthrax. The laboratory worker was one of three employees of Laboratory A who had primary responsibility for processing environmental B. anthracis specimens. Neither this worker nor any of the other approximately 40 employees of Laboratory A had received anthrax vaccine. The laboratory worker did not handle B. anthracis-containing samples or cultures during February 19--28. On February 28, he cut a small bump on his right jaw while shaving, which bled briefly and then became itchy and irritated. On March 1, he assisted a co-worker moving vials containing aliquots of confirmed B. anthracis isolates from the biological safety cabinet (BSC) in the main laboratory to the freezer in an adjacent room. The co-worker had transferred the isolates from blood agar plates to the vials by collecting the growth with a swab. The co-worker removed the vials from the BSC and handed them to the patient. Without gloves, the patient took the vials from the co-worker, placed the vials in the freezer, and then washed his hands with soap and water. During the next 2--3 days, the worker's facial wound increased in size and developed a scab. He also reported right cervical adenopathy, a low-grade fever, and swelling and erythema on his right cheek and neck. The patient's health-care provider obtained a swab of the area underneath the scab and of the area under a vesicle, without cleansing the skin first. The health-care provider made a presumptive diagnosis of cutaneous anthrax and the patient was administered a 2-week course of ciprofloxacin. The culture of this specimen was positive for B. anthracis on testing at Laboratory A and CDC. Because of culture results, the patient was admitted to the hospital on March 5 and treated with intravenous ciprofloxacin and doxycycline pending antimicrobial susceptibility testing. The lesion developed the characteristic eschar of cutaneous anthrax (Figure 1). A chest radiograph performed on admission demonstrated possible fullness of the mediastinum, but computed tomography of the chest was normal. The isolate was susceptible to ciprofloxacin and doxycycline, and the patient continued receiving ciprofloxacin. The patient's symptoms improved during hospitalization, and he was discharged on March 9. Serologic studies for antibodies to B. anthracis are planned. On March 5, Laboratory A's certified industrial hygienist (CIH) performed environmental sampling of both Laboratory A and the patient's residence. Seven wipe samples were taken at the laboratory (i.e., the top of the vials the patient had handled, the key to the freezer where the vials were placed, the doorknob of the freezer room, the centrifuge where specimens are prepared, the two BSCs where specimens are handled, and surfaces in the patient's office in Laboratory A), seven were taken at the patient's residence. The CIH then cleaned surfaces and equipment throughout the laboratory and the patient's residence by using a disinfectant containing a phenolic and a quaternary ammonium compound, which are not sporicidal. The environmental samples were analyzed in Laboratory A. All samples were negative except the wipe sample collected from tops of the vials that the patient had handled, which was positive for B. anthracis. Confirmation of the vial top specimen at CDC is planned. Workers reported that specimen processing of environmental samples suspected of containing B. anthracis is done under Biosafety Level 3 (BSL-3) conditions (1). These samples, including swab, wipe, dust (collected onto filter media by a vacuum), and air samples, are opened in a Class II, Type A BSC in a room designated for acid-fast bacillus specimens (AFB room). Personal protective equipment (PPE) for procedures performed in this room includes disposable, fluid-resistant laboratory coats, gloves, and either a NIOSH-certified N95 or P100 disposable, filtering-facepiece respirator, which are disposed of into a biohazard container before exiting the room. Work with purified B. anthracis cultures is performed in a separate BSC located in the main laboratory room. PPE at this workstation consists of gloves and a laboratory coat. Aliquots of confirmed isolates of B. anthracis are placed in vials and stored in a locked freezer in a room located off the main laboratory. A 10% bleach solution is routinely used to decontaminate surfaces after processing specimens potentially containing B. anthracis. However, because bleach caused labels to become dislodged, storage vials had been sprayed with 70% isopropyl alcohol instead of being wiped with bleach. By the time of the CDC site visit, Laboratory A personnel had obtained labels for storage vials that would not dislodge with bleach. On March 7 and 8, CDC interviewed Laboratory A workers; none reported illness among other employees or their family members. CDC also conducted environmental sampling at Laboratory A on March 7, consisting of 40 surface wipe and 36 air samples. Wipe samples obtained with sterile polyester/rayon pads, moistened with sterile water, were collected from various surfaces in the laboratory and in the adjacent office area, including desks, flooring, door knobs, BSCs, heating, ventilation, air-conditioning return air grills, and laboratory equipment (including the centrifuge and shaker used for processing environmental samples). Air samples were collected in three locations in the laboratory: the AFB room, the area adjacent to the BSC used for anthrax work, and the general microbiology area; two locations in the adjacent office area; and outdoors. All environmental samples were negative for B. anthracis at CDC. On March 8, CDC performed a building assessment, including a ventilation survey, airflow distribution mapping, and BSC characterization. The AFB room was not under negative pressure in relation to adjacent areas of the main laboratory; however, the laboratory was under negative pressure relative to the outside and to the adjacent office areas. The BSCs were functioning adequately. Reported by: TA Mackey, PhD, University of Texas Health Science Center at Houston; EH Page, MD, KF Martinez, MSEE, TA Seitz, MPH, BP Bernard, MD, AL Tepper, PhD, Div of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health; RS Weyant, PhD, Office of Health and Safety; NE Rosenstein, MD, BA Perkins, MD, T Popovic, PhD, Div of Bacterial and Mycotic Diseases; HT Holmes, PhD, Div of Healthcare Quality Promotion, National Center for Infectious Disease; CW Shepard, MD, EIS Officer, CDC. Editorial Note:The findings of this investigation indicate that the worker at Laboratory A likely developed cutaneous anthrax because of skin exposure to a contaminated surface. The health hazard evaluation also identified additional steps Laboratory A should take to ensure worker safety. Because B. anthracis can cause lethal infections and can form infectious aerosols, CDC and the National Institutes of Health recommend that laboratories producing quantities or concentrations of B. anthracis (i.e., culturing the organism for diagnostic purposes) apply practices appropriate to BSL-3 conditions (1). BSL-3 practices emphasize primary and secondary barriers to protect personnel in contiguous areas from exposure to potentially infectious aerosols. A vigorous program of routine decontamination with a 10% bleach solution is needed to kill viable B. anthracis spores on laboratory surfaces and vials. Alcohol is not sufficient to eliminate viable B. anthracis spores from contaminated surfaces (2). Gloves should be used whenever handling material that contains or might contain B. anthracis, and skin defects should be covered with an impermeable occlusive bandage while working in the laboratory. Work should be organized so that all B. anthracis sample manipulations are performed in a single room with most procedures performed in a BSC. Access to such rooms should be limited to laboratorians directly working with the samples. The Advisory Committee on Immunization Practices developed guidelines for routine vaccination with anthrax vaccine (3). This suspected case of laboratory-acquired cutaneous anthrax highlights the need for anthrax vaccination, in addition to standard laboratory safety procedures, for laboratorians who work routinely with B. anthracis specimens. CDC will work with state and local health departments to identify and vaccinate these laboratory workers. This case is defined by CDC as a suspected case of cutaneous anthrax rather than a confirmed case (4) because processing of the swab of the lesion at the same laboratory where the suspected exposure occurred introduces the possibility of contamination of the patient's sample with B. anthracis from the laboratory. However, this patient's clinical syndrome and environmental exposure are consistent with cutaneous anthrax (4). CDC will update the surveillance status of this case as the results of other laboratory tests (e.g., serologic tests) become available. Any exposure leading to a suspected case of cutaneous anthrax requires a public health investigation to identify other exposures in the same setting that might have led to other cases of cutaneous or inhalational anthrax. Local public health authorities should be notified immediately and appropriate laboratory procedures followed when treating clinicians suspect anthrax. This investigation did not identify inhalation exposures, and CDC does not recommend prophylaxis for the prevention of cutaneous anthrax. Active surveillance for cutaneous and inhalational disease should be ongoing among laboratorians working with B. anthracis. AcknowledgmentThis report is based on data contributed by D Mattorano, MS, B King, MPH, D Booher, Div of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 4/4/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 4/4/2002