|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
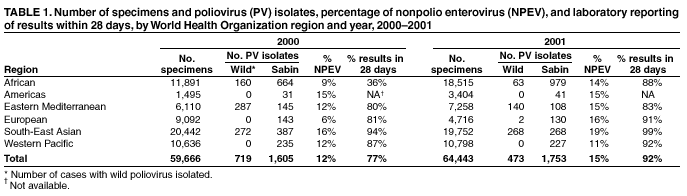
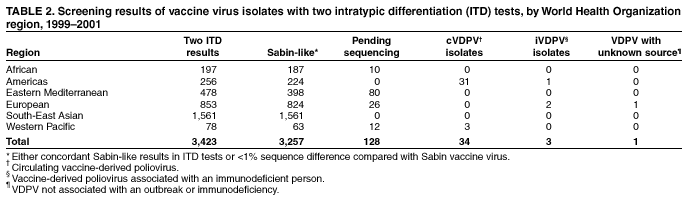
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Laboratory Surveillance for Wild Poliovirus and Vaccine-Derived Poliovirus, 2000--2001After the 1988 World Health Assembly resolution to eradicate poliomyelitis (1), the Global Laboratory Network for Poliomyelitis Eradication (the laboratory network) was established by the World Health Organization (WHO). The laboratory network is one component of the international surveillance system for detecting polio through notification of cases of acute flaccid paralysis (AFP)*. As progress is made in eradicating polio worldwide (2), the laboratory network provides critical virologic evidence about where poliovirus is circulating as a guide to supplementary vaccination activities aimed at interrupting transmission. This report summarizes the laboratory data for documenting the decline in wild poliovirus transmission and the occurrence of vaccine-derived polioviruses and highlights the expanding role of the laboratory network in global polio eradication. In December 2001, the laboratory network was fully operational in all six WHO regions and included 147 laboratories: seven global specialized laboratories, 16 regional reference laboratories, 84 national laboratories, and 40 subnational laboratories in large countries. As of April 2002, a total of 135 (92%) laboratories were fully accredited, six (4%) laboratories were provisionally† accredited, four (3%) laboratories were pending an accreditation review, and two (1%) subnational laboratories had failed to reach accreditation standards. Laboratories are evaluated according to several key performance indicators, including the timeliness of reporting poliovirus isolation results to national programs (i.e., within 28 days of receipt of a specimen) and the nonpolio enterovirus (NPEV) rate, which indicates both an adequate reverse cold chain during specimen transportation and the technical capability of the laboratory to detect enteroviruses. During 2000--2001, the time taken to report virus isolation results decreased, with 92% of results reported within 28 days of receipt of the specimen in the laboratory in 2001 compared with 77% in 2000 (Table 1). Although the number of stool specimens tested increased from 59,666 in 2000 to 64,443 in 2001, the number of polioviruses isolated from AFP cases declined from 719 to 473; substantial disappearance of poliovirus lineages was detected through genomic sequencing. Approximately 10,000 NPEV isolates were identified each year from these stool specimens. Vaccine-derived poliovirus (VDPV) associated with an outbreak of polio (circulating VDPV [cVDPV]) was detected on the island of Hispaniola during October 2000 (3--5). Laboratory network activities were extended subsequently to include screening for these viruses (Table 2), which have acquired wild-like neurovirulence and transmissibility and possess molecular characteristics that differentiate them from either vaccine or wild virus. Since January 2001, all poliovirus isolates are subjected to two methods of intratypic differentiation (ITD): one antigenic and one molecular. Concordant non-Sabin--like ITD results are classified as wild polioviruses, concordant Sabin-like results are classified as Sabin-like (vaccine virus), and any discordant results or Sabin-like isolates lacking two ITD tests are forwarded immediately for sequence analysis of the major viral capsid surface protein (VP1). These isolates are then classified based on the sequencing results: <1% difference from Sabin vaccine virus is classified as Sabin-like, 1%--15% difference is classified as VDPV, and >15% difference is classified as wild virus. The effectiveness of using this approach was demonstrated when three cases of AFP associated with cVDPV isolates were detected in the Philippines during March 2001 (6). In addition to prospective testing, several network laboratories have retested stored vaccine-like poliovirus isolates from before 2001 by using the two ITD methods and subjecting strains with atypical results to further investigation. Of the 3,423 isolates examined to date, 3,257 (95%) were typical vaccine-like viruses and 128 (4%) are pending sequencing results (Table 2). The only highly divergent identified viruses not directly associated with the outbreaks on Hispaniola and in the Philippines have been three polioviruses isolated from immunodeficient persons and one isolate from the Russian Federation in 1999 that had no clear association with an outbreak or immunodeficiency. Reported by: Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Div of International Health, Epidemiology Program Office; Global Immunization Div, National Immunization Program, CDC. Editorial Note:During 2000--2001, the laboratory network initiated genomic sequencing of all wild poliovirus isolates and expanded its mandate to include surveillance for VDPV, which preliminary evidence indicates is rare. Laboratory surveillance conducted by the network documented the interruption of indigenous transmission in the Western Pacific Region (7), the elimination of poliovirus lineages in remaining reservoir countries, and the importation of poliovirus into polio-free countries. In addition to its primary functions of isolation and ITD of polioviruses (i.e., determining wild versus vaccine) from AFP cases (8), the laboratory network provides detailed molecular epidemiologic data on every wild poliovirus isolated within 90 days of onset of paralysis, and often within 60 days of onset in high-priority cases. Genomic sequencing information and close collaboration among network laboratories has allowed the tracking of virus strains within and among countries and the identification of the origin of viruses imported into polio-free countries (9). Timeliness of reporting of stool specimen results improved in all regions during 2000--2001, particularly in the African Region, where the rate more than doubled. Although the expected isolation rate for NPEV can vary widely because of climate, hygiene, and altitude, all regions achieved a rate >10% by 2001. During 2000--2001, the status of the Enterovirus Research Center in Mumbai, India, was upgraded to a Global Specialized Laboratory, and the laboratory in Pyongyang in the Democratic People's Republic of Korea was provisionally accredited. The remaining network laboratories that are not fully accredited have made arrangements to have their specimens processed in parallel in a fully accredited laboratory. In 2001, the Technical Consultative Group on Polio Eradication (TCG) recommended that laboratories reduce the time interval between paralysis onset and reporting of ITD results from 90 days to <60 days and the interval between ITD results and sequencing of wild polioviruses to <28 days. By the end of 2000, almost all reports of wild poliovirus isolation were available within 45 days of receipt of the specimen, and sequence information about almost all critical isolates in 2001 was available within 60 days of receipt of an original stool specimen. Further progress in meeting TCG recommendations will require improved specimen transport among laboratories and more timely analysis and communication of sequencing results. Extending their activities and reducing time intervals has increased the workload of laboratories conducting ITD and sequence analysis, placing substantial pressure on the laboratory network to meet the demands for providing essential reagents for ITD. To ensure that regional reference laboratories are not overburdened, three national laboratories have been accredited to conduct ITD, and several more will be accredited during 2002. Support for laboratories in polio-free areas must continue to ensure early detection of imported wild poliovirus or emergence of cVDPV. The laboratory network is developing and validating methods of supplementary surveillance for polioviruses, including environmental surveillance and enterovirus surveillance. Evidence generated through these methods will be essential for certification of eradication in some areas of the world and for enhanced surveillance and early detection of VDPV after certification. Timely integration of data from the laboratory network into programmatic planning of vaccination responses and identification of the frequency and risk factors associated with cVDPV will be critical for planning in the final stages of the polio eradication effort. All regions will need to continue to support their national and regional laboratories well after interrupting transmission to assure the achievement and maintenance of polio eradication globally. References
* This system is supported by WHO member countries and the Training in Epidemiology and Public Health Interventions Network. † Deficient in one of the areas examined and given a limited time to improve performance before re-assessment.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 5/2/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 5/2/2002