|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
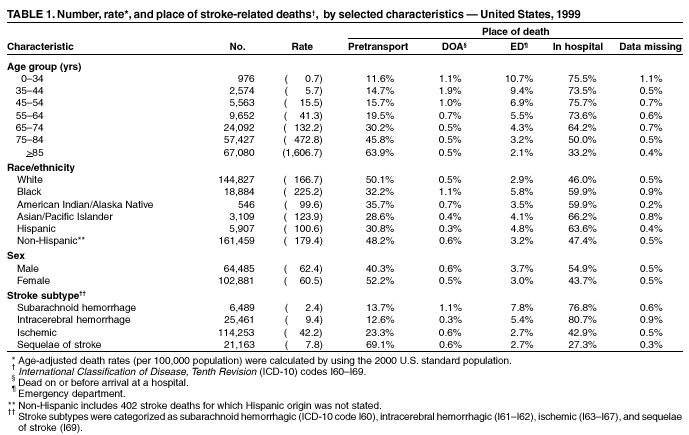
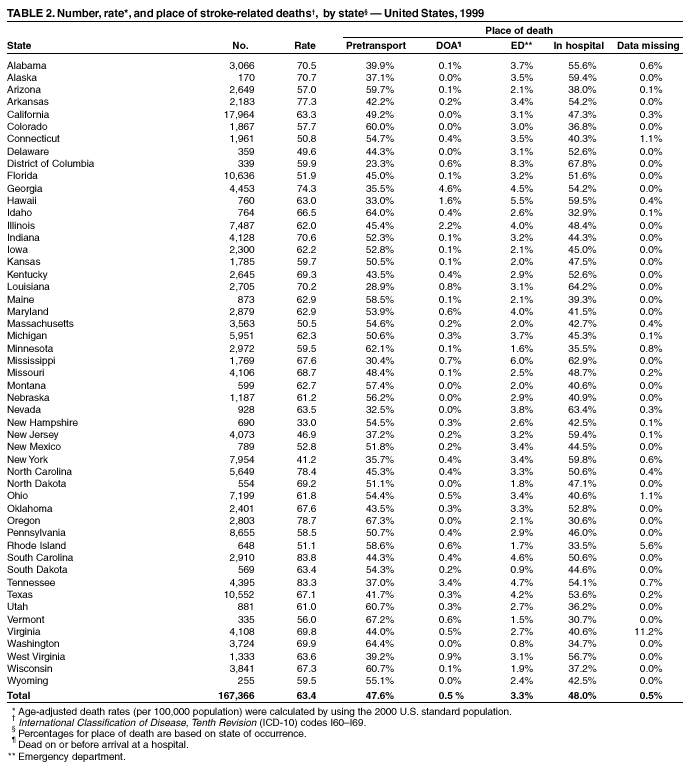
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. State-Specific Mortality from Stroke and Distribution of Place of Death ---United States, 1999In the United States, stroke is the third leading cause of death and one of the major causes of serious, long-term disability among adults. Each year, approximately 500,000 persons suffer a first-time stroke, and approximately 167,000 deaths are stroke-related (1). This report presents national and state-specific death rates for stroke in 1999, which indicate state-by-state variations in both stroke-related death rates and the proportions of stroke decedents who die before transport to an emergency department (ED). Prevention through public and medical education remains a key strategy for reducing stroke-related deaths and disability. CDC compiled national and state mortality data based on death certificates from state vital statistics offices (2). Demographic data were reported by funeral directors or provided by family members of the decedent. Stroke-related deaths are those for which the underlying cause listed on the death certificate by a physician or a coroner is classified according to the International Classification of Diseases, Tenth Revision (ICD-10) codes I60--I69. Stroke subtypes are defined as subarachnoid hemorrhagic stroke (I60), intracerebral hemorrhagic stroke (I61--I62), ischemic stroke (I63--I67), and sequelae of stroke (I69). Place of death was defined as either pretransport, dead on arrival (DOA), in the ED, or in the hospital after admission. Pretransport deaths occurred at the decedent's residence, in a nursing home, or in an extended-care facility before transport to a hospital or ED. Stroke-related death rates for groups defined by age, sex, race/ethnicity, stroke subtype, and state were determined by dividing the number of deaths by the population at risk in that group. Estimates of resident populations and age-adjusted death rates were calculated by using the 2000 U.S. standard population (3). Among U.S. residents, 167,366 stroke-related deaths occurred in 1999, with an age-adjusted rate of 63.4 per 100,000 population. The greatest proportion of deaths occurred among persons aged >85 years (40.1%) followed by those aged 75--84 years (34.3%), those aged 65--74 years (14.4%), and those aged <65 years (11.2%). Age-specific death rates increased for successive age groups (Table 1). By race/ethnicity, the highest age-adjusted death rates for stroke occurred among blacks followed by whites (225.2 and 166.7 per 100,000 population, respectively). Age-adjusted death rates for stroke were slightly higher among men (62.4) than among women (60.5). Ischemic strokes accounted for 68.3% of all stroke-related deaths; age-adjusted death rates were higher for ischemic stroke than for all other stroke subtypes. In 1999, a total of 79,663 (47.6%) stroke-related deaths occurred pretransport, 926 (0.7%) occurred as DOA, 5,519 (3.3%) occurred in the ED, and 80,369 (48.0%) occurred after admission to the hospital; for 889 (0.5%) deaths, place-of-death data were not available. The proportion of pretransport deaths increased with age, and the proportion of deaths that occurred as DOA or in the ED decreased with age. The proportion of pretransport deaths was higher among women (52.2%) than among men (40.3%) and higher among whites (50.1%) than among other racial/ethnic populations. Conversely, the proportion of stroke-related deaths that occurred in the ED was higher among blacks (5.8%) than among other racial/ethnic populations, and higher among Hispanics (4.8%) than among non-Hispanics (3.2%). Compared with other stroke subtypes, the highest proportion of pretransport deaths was among persons who died of sequelae of stroke or other cerebrovascular disease (69.1%), followed by ischemic stroke (23.3%), subarachnoid hemorrhagic stroke (13.7%), and intracerebral hemorrhagic stroke (12.6%). Persons who died of subarachnoid hemorrhagic stroke accounted for the highest proportion of deaths that occurred as DOA or in the ED (1.1% and 7.8%, respectively). The state-specific, age-adjusted death rates for stroke ranged from 33.0 per 100,000 population in New Hampshire to 83.8 in South Carolina (Table 2). The proportion of pretransport deaths ranged from 23.3% in the District of Columbia to 67.3% in Oregon. States with >60% of stroke deaths reported as occurring pretransport were Colorado (60.0%), Wisconsin (60.7%), Utah (60.7%), Minnesota (62.1%), Idaho (64.0%), Washington (64.4%), Vermont (67.2%), and Oregon (67.3%). The proportion of stroke-related deaths reported as DOA ranged from zero to 4.6%; those having occurred in the ED ranged from 0.8% to 8.3%. The proportion of stroke-related deaths for which place-of-death data were missing ranged from zero to 11.2%. Reported by: JE Williams, PhD, CS Ayala, PhD, JB Croft, PhD, KJ Greenlund, PhD, NL Keenan, PhD, LJ Neff, PhD, WA Wattigney, MStat, ZJ Zheng, MD, GA Mensah, MD, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that ischemic strokes account for most stroke-related deaths and that state-by-state variations exist in the proportion of stroke-related deaths that occur pretransport. These findings are consistent with other evidence that many acute ischemic stroke patients cannot benefit from thrombolytic therapy because they do not reach medical treatment in time (4--6). Thrombolytic therapy is a time-dependent therapy with a window of efficacy of <3 hours after the onset of symptoms (4). The reported prehospital delay ranges from 1 to 14 hours, with 3--6 hours as the typical time range (6). Because the advent of thrombolytic therapy has made the early recognition of stroke symptoms and rapid medical response imperative, educational programs are needed for both health-care providers and the public to reduce stroke-related deaths and disability. Educating the public about signs and symptoms of stroke, the need for emergency response (i.e., calling 911), and the importance of immediate transport to an ED might help promote prompt and effective treatment. State-by-state variations in the proportion of stroke-related deaths that occurred pretransport might reflect differences in public awareness of stroke symptoms. Results from population-based surveys suggest that many persons are unaware of the five most common signs and symptoms of stroke: sudden numbness or weakness, sudden dimness or loss of vision, sudden dizziness or loss of balance, sudden severe headache, and confusion or difficulty speaking. Only 57% of survey respondents in the Greater Cincinnati area and 39% in Georgia could identify at least one of these symptoms (7,8). The accurate identification and rapid transport of stroke patients by emergency medical system (EMS) personnel are crucial to the successful early treatment of stroke (9). To assess whether a patient is having a stroke, EMS personnel should be trained properly and equipped with the appropriate technology. In addition, triage nurses and physicians in the ED should be educated to treat stroke as a medical emergency. State-by-state variations in the proportions of stroke-related deaths by place of death might reflect different EMS policies about the need to transport persons who have already died. The high proportion (63.9%) of stroke-related deaths that occurred pretransport among adults aged >85 years might be explained, at least in part, by do-not-resuscitate orders in nursing homes and long-term care facilities, especially for older persons disabled by the sequelae of previous strokes. However, approximately 25% of stroke-related deaths among persons aged <65 years occurred pretransport, as DOA, or in the ED, suggesting that persons in this age group might dismiss stroke as a problem of the elderly and therefore delay their response to symptoms. The findings in this report are subject to at least two limitations. First, data are subject to misclassification of race/ethnicity both in the population census and on death certificates, which might result in overreporting of deaths among blacks and whites and underreporting deaths among other racial/ethnic groups (10). Second, data on underlying cause and place of death are subject to error because they originate from the physicians or coroners who certify each death. Because high blood pressure, diabetes, high cholesterol, and smoking remain the major risk factors for stroke, prevention through public and medical education and through risk-factor reduction should continue to be the focus of public health efforts to reduce the number of stroke-related deaths. Prevention efforts also must include broad-based public health efforts to increase awareness of stroke symptoms and to foster an appropriate and timely response from health-care providers and the public. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 5/23/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 5/23/2002