|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
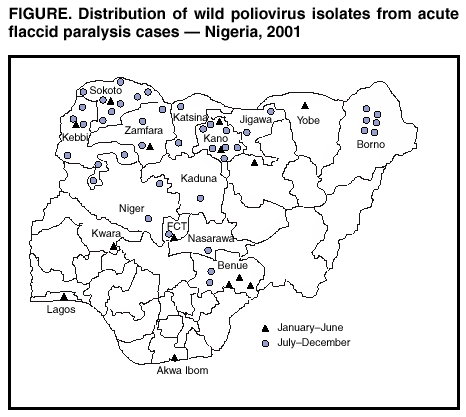
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Poliomyelitis Eradication --- Nigeria, January 2000--March 2002Since 1988, when the World Health Assembly of the World Health Organization (WHO) resolved to eradicate poliomyelitis globally, the annual estimated incidence of polio has declined 99% (1,2). Nigeria is the most populous country in Africa (estimated 2000 population: 127 million) and a major poliovirus reservoir. This report summarizes the progress toward polio eradication in Nigeria during January 2000--March 2002, highlighting achievements in acute flaccid paralysis (AFP) surveillance and evidence indicating reduced poliovirus transmission. The findings underscore the importance of ensuring a rapid flow of surveillance information to guide program activities. Few health facilities in Nigeria provide routine vaccination services on a regular basis. In 2000, administrative data suggested that 38% of the estimated number of infants aged <1 year had received 3 oral polio vaccine (OPV) doses, and a survey of vaccination cards or histories of children aged 12--23 months suggested 24% coverage; no data are available for 2001. Problems identified in the routine vaccination system include inadequate vaccine transport and cold chain system at local government area (LGA) and health-facility levels, inadequate monitoring and supervision of routine vaccination activities, and irregular vaccine procurement at the service-delivery level. Plans to strengthen routine vaccination at the LGA level are under way. With the support of WHO and the United Nations Children's Fund (UNICEF), the country has developed a 5-year cold chain rehabilitation plan. Supplemental OPV vaccination activities targeting children aged 0--59 months have been conducted annually in Nigeria since fixed-post National Immunization Days (NIDs)* were begun in 1997. To improve coverage, in 1999, NIDs were modified to be exclusively house-to-house, and extra rounds of sub-National Immunization Days (SNIDs) were added. Supplementation with Vitamin A, occurring twice yearly with NIDs, began in June 2000. During 2000, SNIDs reached 6,633,798 children in June and 7,417,616 children in July, and NIDs reached 42,254,312 children in October and 44,306,277 children in November. During 2001, NIDs reached 46,881,439 children in January, 39,336,362 children in April, 39,336,808 children in June, and 34,778,783 children in November. Because of an OPV shortage, SNIDs were conducted in October 2001 instead of NIDs; this round reached 19,318,407 children in high-risk areas. Estimated OPV coverage of the target population during 2001 was 88%--98%. In the fourth round, approximately 700,000 children with no previous OPV dose were reached. NIDs during October--November 2000 and November 2001 were synchronized with those of other countries in western and central Africa with substantial cross-border vaccination activities (3). AFP surveillance quality is evaluated by two key indicators: sensitivity of reporting (target: nonpolio AFP rate of >1 case per 100,000 children aged <15 years) and completeness of specimen collection (target: two adequate stool specimens from >80% of all persons with AFP). In 2000, a joint team comprising national and international experts assessed polio-eradication activities in Nigeria and developed a 5-year strategic plan. The team recommended that at least one dedicated AFP surveillance officer be assigned per 3,000,000 population. By September 2000, after having been recruited and trained in AFP surveillance, these officers assumed full-time responsibility for AFP surveillance. During 2001, an intermediate-level supervisory structure was introduced. During 2000--2001, the national AFP case detection rate increased from 1.0 per 100,000 children aged <15 years to 3.5, the nonpolio AFP rate increased from 0.6 to 2.2, and the adequate stool specimen collection rate increased from 35% to 65% (Table). In 2001, in all 36 states plus the Federal Capital Territory (FCT) of Abuja, the nonpolio AFP rate was >1.0; for all AFP cases, at least one stool specimen was collected within 28 days. In seven states, collection of two adequate stool specimens was <60%. During January--March 2002, two adequate stool specimens were collected for 85% of AFP cases; 27 (73%) states had a rate of >80%, seven (19%) had a rate of 60%--80%, and three (8%) had a rate of <60%. The AFP surveillance system is supported by two national WHO-accredited laboratories, one located in Ibadan in Oyo State and the other in Maiduguri in Borno State. During 2000--2001, the number of stool specimens processed by these laboratories increased from 1,940 to 3,821. An indicator of the quality of the reverse cold chain for transport of stool specimens to the laboratory is the isolation rate of nonpolio enteroviruses (NPEV); the target rate is >10%. In 2001, the NPEV isolation rate was 7.7%. During January--March 2002, the NPEV isolation rate was 10.2%. Improvements in AFP surveillance were associated with an increase in the number of wild poliovirus isolates detected, from 29 (28 type 1, one type 3) in 2000 to 56 (35 type 1, 21 type 3) during 2001. Genetic sequencing data from polio-viruses isolated indicate that lineages are disappearing, suggesting declining intensity of transmission. Surveillance data showed a shift in the geographic distribution of wild polio-virus transmission to the northern states during July--December 2001 (Figure). Genetic sequencing data showed that polioviruses isolated during 2001 from persons with AFP in neighboring southern Niger were of Nigerian origin (2). As of March 31, 2002, a total of 10 polioviruses have been isolated in seven states and Abuja FCT(two each from Kano and Katsina, and one each in Niger, Kaduna, Abuja FCT, Gombe, Jigawa, and Borno), all areas in which polio was identified as highly endemic in 2001. During 2001, of 56 confirmed cases, 29 (52%) were among children aged 24--59 months, 20 (35%) were among children aged 12--23 months, and seven were among infants aged <12 months. Of 22 children whose vaccination status was known, eight (36%) had received 1 OPV dose, and seven (32%) had received 2 OPV doses. Reported by: Federal Ministry of Health, Abuja, Nigeria. Vaccine Preventable Diseases, World Health Organization Regional Office for Africa, Harare, Zimbabwe. Vaccines and Biologicals Dept, World Health Organization, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:During 2000--2001, AFP surveillance improved substantially in Nigeria. The genetic sequencing data from polioviruses isolated suggest elimination of multiple genetic lineages and greatly reduced intensity of transmission. In parts of southern Nigeria, no wild polioviruses have been isolated since July 2001. Transmission continues in the northwestern states (type 1) and the northern central and northeastern states (type 3). Key achievements over the past 2 years include creation of an expanded AFP surveillance medical officer infrastructure covering all parts of the country, implementation of an intensified house-to-house vaccination strategy during NIDs and SNIDs, and supplementation of hundreds of thousands of children with vitamin A during polio vaccination campaigns. Despite progress, Nigeria remains one of the three global poliovirus reservoirs (along with northern India and Pakistan) whose low routine OPV vaccination coverage and high population density favor poliovirus transmission. A joint national/ international review in February 2002 highlighted several remaining challenges to eradicating polio in Nigeria. The review team found inadequate management of supplemental vaccination activities at the LGA level and recommended improvements in NID planning, vaccinator training, and day-to-day monitoring of vaccination activities. The team also found consistent delays in paying vaccination teams, leading to considerable lack of motivation and children being missed. Despite substantial progress in AFP surveillance, further improvements are needed in the geographical representativeness of surveillance quality indicators and the NPEV rate to ensure that poliovirus transmission is not occurring undetected. Finally, improved social mobilization efforts are needed to target members of ethnic minorities and other high-risk groups that are missed frequently by supplemental vaccination activities. In 2002, AFP surveillance data are being used to target SNIDs more precisely. Two rounds of SNIDs were implemented during April--May 2002 in areas in which wild poliovirus isolates were identified during July--December 2001. Responsive mop-up vaccination will occur immediately following the detection of any poliovirus in Nigeria; this will require the rapid flow of surveillance information to guide program activities. A group of national and international experts will meet in summer 2002 to review the epidemiologic situation and make additional recommendations. NIDs are planned for September and November 2002. Implementation of these activities will enable Nigeria to interrupt transmission of wild poliovirus. References
* Mass campaigns over a short period (days) in which 2 doses of OPV are administered to all children in the target group (usually those aged <5 years) regardless of previous vaccination history.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 6/6/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 6/6/2002