|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
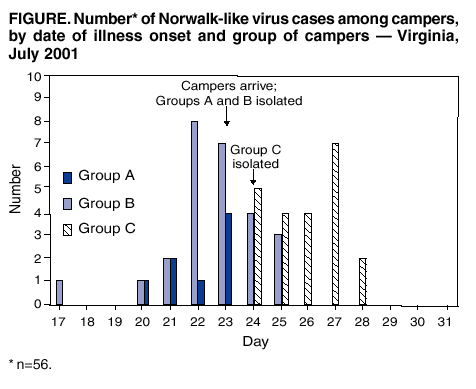
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Norwalk-Like Virus--Associated Gastroenteritis in a Large, High-Density Encampment --- Virginia, July 2001Norwalk-like viruses (NLVs) are an important cause of gastro-enteritis in the United States, with approximately 23 million cases of NLV-associated gastroenteritis occurring each year (1). NLVs accounted for 96% of nonbacterial gastro-enteritis outbreaks reported to CDC during January 1996--June 1997 (2). These outbreaks are common especially in settings of crowding and poor sanitation (2,3). Transmission of NLVs in these settings is facilitated by high attack rates (82%) (4), a low infectious dose (<100 virions), the absence of long-lasting immunity, the durability of the organism (5), and the potential for multiple modes of transmission (3,6). In 2001, outbreaks were reported from youth camps in Wisconsin and Florida, resulting in closure of the camps (7; CDC, unpublished data, 2001). This report describes an outbreak of NLV-associated gastroenteritis at a large youth encampment in Virginia and the successful use of control measures to limit spread of illness to other campers. Rapid, effective containment is a central goal of public health response when outbreaks of infectious diseases occur. In July 2001, a large encampment held every 4 years by a national youth organization began in rural Virginia. Approximately 40,000 campers arrived on July 23 from locations throughout the United States and from several other countries. The camp was divided into 20 subcamps comprising approximately 600 groups of 40--90 campers, who were housed in tents. Groups of campers shared water that was dispensed at multiple central locations, outdoor showers, and flush toilets that drained to septic systems. Meals were prepared in small groups of five to 10 campers. On arrival, each group of campers had a requisite health-screening examination before proceeding to a campsite. Medical and public health personnel screened each group by using a standard interview form that asked about the presence of rashes, vomiting, diarrhea, fever, headache, and cough. Groups of campers in which at least one person had a rash or at least two persons shared other symptoms associated with communicable disease were then referred for in-depth screening by the epidemiology support team. Ill campers were asked about the nature and timing of symptoms, travel history, and the source of food and beverages consumed recently. In addition, campers from each of the 20 subcamps within the 7-square-mile encampment who had vomiting, diarrhea, or other symptoms were assessed daily during the encampment to monitor for outbreaks of illness. On initial screening, two groups of campers had multiple members with vomiting and diarrhea. Initially, these symptoms were found in six (8%) of 80 campers in group A from Illinois and 15 (18%) of 84 in group B from California; both groups arrived on July 23. On the morning of July 24, five (6%) of 80 members of group C from Oklahoma, camped several miles from the other two groups, were found to have similar symptoms. All illnesses were characterized by an acute onset of malaise, nausea, vomiting, and diarrhea. Symptoms typically lasted 24--48 hours. Review of cases by date of onset suggested an infectious illness that had an incubation period of approximately 24 hours but was inconsistent with a single-point source for all of the outbreaks (Figure). Attack rates were eight (10%) of 80 for group A, 26 (31%) of 84 for group B, and 22 (28%) of 80 for group C. Interviews of patients did not reveal any shared exposures or travel history among the three groups. Stool samples were collected from two (25%) of eight ill campers in group A, two (8%) of 26 ill campers in group B, and four (18%) of 22 ill campers in group C. NLVs were detected by the Virginia Division of Consolidated Laboratory Services by using reverse transcriptase-polymerase chain reaction (RT-PCR) in six of the eight stool samples, two from each group. All strains were tested at CDC and were genetically identical within the portion of the genome sequenced. Control measures, including limiting contact between ill and well persons, were instituted for groups A and B on July 23 and for group C on July 24. All members of groups in which cases of gastroenteritis had been identified were excluded from camp activities in which transmission might occur, including all water sports and any activity in which a shared implement might be contaminated (e.g., archery, shooting, and rappelling). Affected groups were provided with dedicated latrines and washing facilities and were supplied with drinking water, ensuring that they would not draw it themselves from sources used by other campers. Shower space was reserved for affected group members at specified times; facilities were cleaned after each use with a 10% bleach solution. All symptomatic campers were excluded from food handling or preparation for at least 48 hours after resolution of symptoms. Scrupulous hand washing was stressed for all members of the affected groups. Arrangements were made so that well members of affected groups could participate in limited camp activities consistent with enteric precautions (e.g., supervised walks around the encampment and attendance at evening concerts). An affected group was released from isolation when no new cases in that group were detected for at least 36 hours; however, campers remained in isolation until they were asymptomatic for 48 hours. Outbreaks in the affected groups lasted 4--9 days, compared with durations of 3--4 weeks in two recent camp-associated outbreaks (7; CDC, unpublished data, 2001). Group A was released from isolation on July 25, group B on July 26, and group C on July 29. No new cases were reported from any of the three groups between the time of release from isolation and the end of the encampment. Of 244 campers in the three groups, 56 (23%) became ill. For the subcamps housing the three affected groups, the average rate of campers who had vomiting or diarrhea was 6.0 per 1,000 campers, compared with 3.7 among nonaffected subcamps. On July 31, the final evening of the encampment, 36 campers staying at the same subcamp as group A became ill with vomiting or diarrhea, for a rate that day of 23.3. Because all campers left the next morning, no information was available on the group or groups involved. The sudden increase in gastrointestinal symptoms was indicative of a point-source outbreak; rates for such symptoms at the subcamp during the days between this outbreak and the release of group B for general activity had averaged 4.1 with no significant upward trend. Reported by: JE Cheek, MD, P Young, Indian Health Svc, California area. L Branch, Virginia State Dept of Health; KM Dupnik, ST Kelly, JM Sharp, DM Toney, PhD, Virginia Div of Consolidated Laboratory Svcs. JS Bresee, MD, SS Monroe, PhD, RS Beard, S Bulens, MPH, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; R Leman, MD, EIS Officer, CDC. Editorial Note:The findings in this report suggest that intervention efforts were effective in limiting spread of disease within and among groups. However, because no formal control group was available for comparison, the effectiveness of the control measures cannot be proven, given the opportunities for NLV transmission in this crowded, primitive camp setting. The control measures were designed to mitigate foodborne, waterborne, and person-to-person spread. Isolating affected groups and providing dedicated latrines and washing facilities decreased the likelihood of person-to-person or fomite-mediated spread to noninfected groups. Within affected groups, avoidance of food handling by infected campers and frequent hand washing were apparently effective in limiting transmission to other group members. Although evidence of NLV viral shedding has been noted by RT-PCR testing as late as 2 weeks after symptom resolution (8), use of a shorter isolation period appears to have been effective in controlling this outbreak. The sudden increase in gastroenteritis cases among campers in the vicinity of group A suggests a point-source exposure that might not have been related to NLV. However, no specimens were available for testing, and the number and identity of groups affected by this late outbreak were unknown. The absence of any additional cases among group A campers and of any identifiable outbreaks among other groups in the subcamp during the intervening 6 days between group A's release and the final outbreak suggest that the original outbreak was not linked directly. Although several outbreaks of NLV gastroenteritis in bivouac or military base settings have been reported (7,9; CDC, unpublished data, 2001), the effectiveness of possible control measures is not known. Although closure of camps was required to end transmission in two recently reported NLV outbreaks in camp settings (7; CDC, unpublished data, 2001), disease was apparently contained at the Virginia encampment, even though the nonisolated camper population was 20 times larger. Factors critical to the successful containment of this outbreak include: 1) the preparations of local public health staff, who had an effective control system in place before the campers arrived; 2) the diligence of affected campers, whose compliance was induced by incentives to participate in activities available to nonisolated campers at this event; 3) active surveillance; and 4) prompt implementation of control measures. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/1/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 8/1/2002