|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
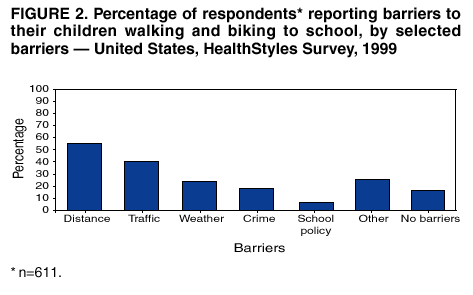
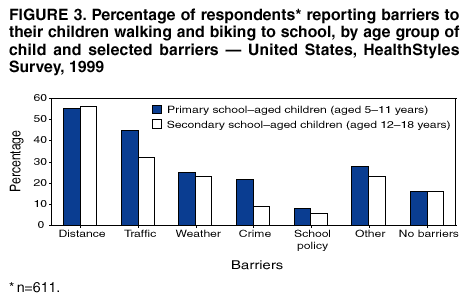
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Barriers to Children Walking and Biking to School --- United States, 1999Physical activity is an important part of a healthy lifestyle; however, many children in the United States do not meet recommended levels of physical activity (1). Although walking and biking to school can increase physical activity among children, motor-vehicle traffic and other factors can make these activities difficult. The majority of U.S. children do not walk or bike to school, approximately one third ride a school bus, and half are driven in a private vehicle. Less than one trip in seven is made by walking or biking (2). To examine why the majority of children do not walk or bike to school, CDC analyzed data from the national HealthStyles Survey. This report summarizes the results of that analysis, which indicate that long distances and dangerous motor-vehicle traffic pose the most common barriers to children walking and biking to school. Public health and community-based efforts that encourage walking and biking to school should address these barriers (Figure 1). CDC provides technical assistance to Porter/Novelli (Washington, D.C.) in conducting the HealthStyles Survey, an annual mail survey of health-related attitudes and behaviors in the United States. In 1999, investigators solicited 3,550 households that had previously indicated a willingness to respond to survey questions. This sample was selected as representative of the U.S. population on the basis of eight demographic variables: age, sex, marital status, race/ethnicity, income, region, household size, and population density. A total of 2,636 (74%) households responded; the 749 (28%) households with children aged 5--18 years were asked 1) if their youngest child walked or biked to school at least once a week during the preceding month, and 2) whether any of six specified conditions made it difficult to do so: traffic danger, crime danger, long distances, weather, opposing school policy, or other reasons. Respondents also had the option of stating that their children had no barriers to walking or biking to school. Results were weighted to match population distribution in the United States by using the eight demographic variables. Of the 611 respondents, 19% reported children walking and 6% reported children biking to or from school at least once a week during the preceding month. Frequency of walking and biking trips ranged from zero to >10 times a week (mean frequency: six one-way trips a week). These trips represented 14% of all school trips (11% walking and 3% biking). The proportions of primary school--aged children walking (18.6%) and biking (5.7%) to school were similar to those of secondary school--aged children walking (19.6%) and biking (5.7%) to school. Reported barriers to walking and biking to school included long distances (55%; 95% confidence interval [CI]=+4%), traffic danger (40%; 95% CI=+4%), adverse weather conditions (24%; 95% CI=+3%), crime danger (18%; 95% CI=+3%), opposing school policy (7%; 95% CI=+2%), or other reasons (26%; 95% CI=+3%) (Figure 2). A total of 16% (95% CI=+3%) reported no barriers to their children walking or biking to school. Of the 16% of respondents who reported no barriers, 64% reported children walking, and 21% reported children biking to or from school at least once a week during the preceding month. Children with no barriers were six times more likely to walk or bike to school than the rest of their peers aged 5--18 years with one or more barriers. A total of 66% of the children were primary school--aged (aged 5--11 years); 34% were secondary school--aged (aged 12--18 years). Reported barriers for primary school--aged children were compared with those for secondary school--aged children (Figure 3). Proportions were similar for distance, weather, opposing school policy, and other reasons. The proportion of respondents reporting no barriers to their children walking or biking to school was the same for both age groups. However, primary school--aged children reportedly faced barriers of traffic danger and crime danger significantly more than their older peers. Reported by: AM Dellinger, PhD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control; CE Staunton, MD, EIS Officer, CDC. Editorial Note:To increase physical activity among children, two of the national health objectives for 2010 are to increase the proportion of trips to school made by walking and biking (objectives 22-14,15) (3). The median distance to school from a child's residence is relatively long (2 miles for children aged 5--15 years); however, many children do not walk or bike to school even when distances are short. For children living <1 mile from school, only 31% of trips are made by walking, and for children living <2 miles from school, only 2% of trips are made by biking (3). Results from the HealthStyles Survey indicate that approximately two thirds of children walk or bike to school when barriers are not present; however, the majority of parents report that their children face barriers to walking and biking to school. Substantial resources, diverse expertise, and ongoing political commitment are required to address the two most important barriers: long distances and traffic danger. Traffic danger inhibited approximately 40% of children from walking or biking to school. When extrapolated to the U.S. population, these findings indicate that perceived traffic danger prevents approximately 20 million children from walking or biking to school (4). Additional data indicate that perceived traffic danger is an understandable concern. Although U.S. children aged 5--18 years walk relatively little and bike even less, approximately 550 pedestrian deaths and 250 cyclist deaths occur annually among this population (5), and approximately 100 nonfatal injuries occur for each death (6). The findings in this report are subject to at least two limitations. First, the HealthStyles Survey solicits a population identified by its willingness to participate in survey research. Second, approximately 18% of respondents with children did not respond to questions about walking and biking to school. This pool of respondents might not represent the overall attitudes and behaviors of U.S. households. Improving traffic safety is crucial for programs that encourage children to walk or bike to school. To advance local pedestrian and cyclist safety initiatives, CDC research and surveillance data have been used to 1) formulate guidelines for age-appropriate child-pedestrian supervision (7), 2) support bicycle-helmet promotion, and 3) outline national strategies for advancing both child-pedestrian and bicycle safety (8,9). Many U.S. communities are facilitating walking and biking to school by addressing traffic safety concerns, mapping safe routes to local schools, building new schools in residential neighborhoods, and involving parents in programs such as Walking School Bus, Bike Trains, and Walk to School Day. The Marin County Safe Routes to School program in California is an ongoing effort developed by the Marin County Bicycle Coalition, funded by the National Highway Traffic Safety Administration and other state and local sources, and assisted by numerous parent volunteers. The Marin County program reported a 57% increase in walking and biking to school in its first year (10). Efforts focused on creating safe and accessible routes for children walking and biking to school promise the additional benefit of producing neighborhoods that ensure safer walking and biking for all ages. Additional information about programs and resources for promoting safe walking and biking to school is available at the following websites: http://www.cdc.gov/nccdphp/dnpa/kidswalk/fact_sheet.htm and http://www.cdc.gov/ncipc at CDC, http://www.walktoschool-usa.org at Walk to School Day---USA, and http://www.safekids.org at the National SAFE KIDS Campaign. Acknowledgments The data in this report are based on responses to the HealthStyles Survey developed by Porter/Novelli in collaboration with the Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/15/2002
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 8/15/2002