|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
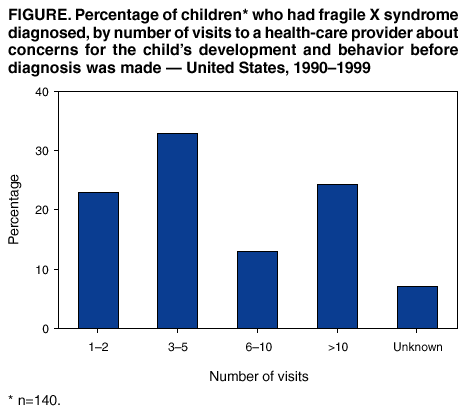
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: [email protected]. Type 508 Accommodation and the title of the report in the subject line of e-mail. Delayed Diagnosis of Fragile X Syndrome --- United States, 1990--1999Fragile X syndrome (FXS) is the leading cause of inherited mental retardation, affecting approximately 50,000 persons in the United States (1). FXS occurs when a mutation on the X chromosome is passed from mother to child. Preliminary data suggest that children affected by FXS experience a delay in diagnosis, a pattern common to other single-gene disorders (2). The molecular test used to definitively diagnose FXS became available in 1991. The first indication of FXS within a family is usually the diagnosis of FXS in a child. Although no proven treatments exist for FXS, prompt diagnosis enables children to receive early intervention services and families to receive genetic counseling (3,4). To assess the timing of a diagnosis of FXS in an affected child and genetic counseling for the family, the Frank Porter Graham Child Development Institute (University of North Carolina at Chapel Hill) conducted a survey during August--October 2001 of 140 parents whose first child affected by FXS was born and had the condition diagnosed during 1990--1999. This report summarizes the results of that survey, which indicate that approximately half of the families did not learn the diagnosis for more than a year after first concerns about their child's development or behavior, and half reported having subsequent pregnancies before FXS was diagnosed in their first child. These findings emphasize the importance of increased opportunities for early diagnosis so children and families can receive all possible benefits, including genetic counseling and intervention services. No population-based registries for FXS exist in the United States, and few children are identified by routine surveillance systems for birth defects and developmental disabilities. To gather an adequate number of families in a short time frame, investigators used a convenience sample from mailing lists of research institutions and parent-based groups. The families surveyed were identified through two sources: the Carolina Fragile X Project, comprising families in the southeastern United States ascertained for a longitudinal cohort study of FXS (2), and the FRAXA Research Foundation, a parent-based group focused on FXS education and research. The questionnaire asked about the process of finding out about the FXS diagnosis and the impact of the diagnosis on the family. Each parent of a child with FXS was asked to complete the questionnaire, with the assurance that answers were confidential and could not be linked to names. Approximately 535 questionnaires were mailed, and 460 questionnaires representing 299 distinct families were completed. If both parents from the same family responded, the mother's questionnaire was chosen for analysis. Nonbiologic parents (n=nine), parents who knew their FXS carrier status before the index pregnancy (n=16), and parents whose children were born before 1990 (n=134) were excluded; 140 families (126 boys) were included in the survey. At the time the questionnaire was completed, the mean age of the 140 respondents was 37.6 years (standard deviation: 5.8 years); 93% of the respondents were white, 61% had completed at least an undergraduate degree, and 37% had an annual household income >$100,000. Before becoming pregnant with the first child affected by FXS, 40 (29%) of 139 respondents knew that they had a family history of mental retardation, learning problems, or behavioral problems. In this sample, all children had FXS diagnosed after birth when symptoms began to develop. After the first contact with a health-care provider, 34 (24%) of 140 respondents reported visiting a health-care provider about the child's development >10 times before the genetic test for FXS was ordered (Figure). Because girls with FXS might have less distinct physical features, historical endpoints were calculated only for boys. A substantial gap existed between the child's age at the time someone became concerned about the child's development or behavior (median age: 12 months; range: 0--50 months) and the child's age at diagnosis of FXS (median age: 26 months; range: 6--101 months). For many parents, the delay between the birth of the child and FXS diagnosis precluded informed reproductive decisions. Of the 140 parents, 70 (50%) reported having another child before their first child had FXS diagnosed; of these 70 parents, 30 (43%) had another child affected by FXS before the first child had FXS diagnosed. Overall, 124 (89%) of 139 parents reported receiving genetic counseling, and 99 (73%) of 136 reported that the diagnosis affected their decision to have another child. When parents were asked to choose the best time to offer voluntary genetic testing for FXS, 103 (75%) of 138 indicated that the best time would be before a woman becomes pregnant. Reported by: DB Bailey, PhD, D Skinner, PhD, K Sparkman, Frank Porter Graham Child Development Institute, Univ of North Carolina at Chapel Hill. CA Moore, MD, RS Olney, MD, National Center on Birth Defects and Developmental Disabilities; DC Crawford, PhD, EIS Officer, CDC. Editorial Note:This report documents both the occurrence of a delayed diagnosis for a child with FXS and the impact this delay has on family planning. Early identification provides benefits for both the family and the affected child. First, early identification provides parents with a diagnosis, potentially reducing the psychosocial impact they face in searching for the cause of their child's disorder and providing more impetus for participation in early intervention programs. Second, early identification could provide parents an opportunity to receive genetic counseling for family planning. Third, early identification would allow the child to receive available intervention services. Infants who have FXS diagnosed are immediately eligible for publicly funded developmental services (e.g., early intervention programs) in all 50 states under Part C of the Individuals with Disabilities Education Act (5). Finally, early identification allows researchers to better understand the natural history of the disorder and provides an opportunity for testing the effectiveness of new interventions (5). Despite the potential benefits of early identification, strategies for obtaining an early diagnosis in a child are limited. Two such strategies are newborn screening (3,6,7) and early clinical recognition (8,9). Adding disorders such as FXS to newborn screening programs would guarantee a timely diagnosis. However, FXS does not have a proven treatment that must be administered shortly after birth, which is the fundamental criterion used to justify rapid, universal identification of a disorder in a newborn (3,6). Similarly, the clinical screening strategy might not be optimal for early identification of disorders such as FXS. The signs for FXS clinical recognition often are subtle, and no single factor (e.g., severity of mental retardation or behavior) is associated with the variability in the length of time from a child's birth to diagnosis of FXS (5). Strategies to enhance early clinical identification of FXS could include education programs for health-care providers that emphasize the importance of developmental screening and ascertaining family history as part of routine well-child health care, and focusing on improved recognition of the signs and symptoms of FXS and other developmental disorders in young children. The findings in this report are subject to at least two limitations. First, the convenience sample used for this survey probably does not represent all families affected by FXS in the United States. Respondents were parents who have elected to participate in research in the past or have an active interest in research and policy concerning FXS. Second, because the analyses were limited to a specific time frame, the sample size was relatively small. Despite these limitations, this survey documents the consequences of a delayed diagnosis of FXS for both the child and the family. Although the strategies to obtain an early diagnosis for disorders such as FXS are limited, new approaches are needed to optimize access to services and information for personal health decisions and family planning. References
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to [email protected].Page converted: 8/22/2002 |
|||||||||
This page last reviewed 8/22/2002
|